Health Psychology
How Legal System Shortcomings Fail Domestic Violence Victims and what we may learn from these failings
WESTBOROUGH, MA – October 31, 2024 – I am writing in the aftermath of another murder suicide here in Massachusetts. It happened 3 months ago at the end of the school year. An adolescent girl was walking home from school and was abducted by her former step-father who is charged with raping her when she was 13. He was wearing an ankle bracelet designed to provide police with GPS coordinates when he deviated from going to and from his work place or if he deviated anywhere near the victim from whom he had a stay away order. Technically, as soon as he drove near the childs school or home the police should have been notified. But this did not happen and now the girl and the former step-father are dead. I have written to the Middlesex County district attorney here in Massachusetts about this case with ideas I have about domestic violence homicide and best practices, but so far, I have heard nothing back. I presume they have all the expertise and advice they require to help keep people safe from trolls and jealous spouses with outstanding orders of protection.
I am a former police sergeant and have looked at several cases each year that are compelling and I try to report these. I asked the local chief of police for the police reports on this case but was sent only the press release. My interest started both from my experience in law enforcement and also out of a response to the abject horror the so many of these cases, like this one. People living in fear, month after month, or in some cases years of fear. This case was delayed over and over. A common tactic used by defense attorneys to avoid going to trial at all. They are banking on the victim being too frightened to testify or better yet, the victim moves away and cannot be found. Victim witness advocates will tell you that teenaged children carry a great deal of shame with them after being victimized. Every delay or change in court dates can trigger fear and often self-doubt. Many know the protection orders have very little that prevents a stalking step-parent from wreaking terror on his victim and her family. In this case, the restraining order failed the victim in spite of the best efforts of law enforcement with things like old technology GPS monitoring.
This case flew under the radar because the criminal trial of the accused was re-scheduled 3-4 times over several years. It was finally headed toward the court room and it is a fact, that as this occurs the risk to potential victims increases as domestic violence cases plod toward a trial. Every change in court date is enough to put a frightened victim into crisis. Many if not most, victims of DV change their minds and do not prosecute. They often blame themselves for breaking up the family by coming forth with sometimes horrific accusations as in this case. In the long run, this impacts their emotional development and victims should be afforded all the support they require to be capable of going to trial. They often are too afraid to stand up and admit what was done to them. They feel shame and deeply frightened.
As I said, I am a former police officer and currently MA licensed psychologist working in here in Massachusetts. When I patrolled the town, I frequently stopped at houses known to us for domestic violence calls in the days afterward. I sometimes had one of our community policing officers with me in the aftermath of the call. When everything was settled down and the dust had cleared, I would stop and try to connect with the couple. Follow-up on recommendations I may have offered – like family or couples therapy and other local resources. And let them know help is available. I was surprised at how many families moved away soon after being involved in a family fight. Off my radar right? My understanding of domestic violence is that it cycles from guilt and shame to honeymoon and a family love fest. The cycling of coercive, violent behavior ramps up one a trial nears or some other dramatic change like divorce. These are the most dangerous times and any violations once the GPS monitor is in place should require arrest with no bail. While in containment, the psychological assessment must be initiated and presented to the court.

The double dose of the stigma of both suicide and intimate partner violence (IPV) leaves the details of many of these traumatic experiences untold.
Everytown Research and Policy, 2024
“These tragedies often include children, family members, and friends.” Despite the devastation and immeasurable impact, these events garner little public attention and recognition as a frequent form of gun violence.” according to a story published on 8-8-2024. More needs to be done to protect child victims from known violent perpetrators such as Juliano Santana, who killed a 16-year-old girl a few weeks ago in Acton, Massachusetts. Child victims like the 13-year-old victim in this case often blame themselves for being physically assaulted or being groomed for sexual assault. They lack the developmental and emotional maturity to fully understand what has happened to them and often live in recurring fear that the rapist is going to come back and hurt them again or kill them next time. The media portrayal of these horrific events failed to ask the important question how did the perpetrator avoid being captured before he got to his one-time stepdaughter? He was attached to a GPS device, right? And where did he get the firearm used to kill the teen and turn it on himself? Well, it sounds as though the police have determined that the GPS may be partially to blame. As soon as they queried the device, they knew Santana was on the move and the victim was grave danger. And where did the deadly firearm come from?
“Access to a gun is the centerpiece of the dual tragedies of intimate partner homicide and suicide.”
The GPS ankle monitor system did not protect the victim because it was not the type of monitor that would alert law enforcement when a suspect diverts from his programmed daily route or if he drove near the school or apartment complex where the victim lived. So, after 3 years the trial was set to begin in July 2024. That is usually a red flag and signals growing anxiety in both the victim and the suspect. Under state law, prosecutors cannot request a hearing to determine if someone is dangerous or whether he should be held in cases involving egregious cases of child rape. The rape of a child is de facto evidence of dangerousness in most circles.
As a former law enforcement officer and a now licensed psychologist here in Massachusetts and I have looked at DVH. I find it necessary to draft reports that highlight the murderer’s unpredictable violence. Certainly, the probation department looks at the perpetrator’s prior criminal history in making recommendations for bail. It is likely that Mr. Santana had no criminal history although we have not been told this fact. Juliano Santana drove to Acton with one thing in mind – to shoot and kill the 16-year-old girl whom he first violated 3 years prior when she was just 13. He should have been in a holding cell until he received a dangerousness assessment.
“Law enforcement agencies should implement a lethality risk assessment protocol in domestic violence cases that includes instructing officers to ask about the presence of firearms and other known risk factors for lethal violence.”
There is nothing more frightening than to be the person who asks for a restraining order for protection from a monster that allegedly raped her as a 13-year-old girl. She was not his biological daughter. How is it possible that someone who has demonstrated such violent and dangerous behavior cannot be held until his dangerousness can be assessed? Here in Massachusetts conditions of bail have no bearing on criminal behavior once released. Bail does not stop secondary criminality. The likelihood of terminal violence such as this, is extremely high as the court begins to move on the case. Santana skidded through the pervious gauntlet and killed his victim and then himself. Rather than say that there were many things in place to protect the victim, there needs to be an investigation as to how the protection order failed? This case is an abject failure.
More needs to be done to protect child victims from known violent perpetrators. News reports say there were things being done to protect the victim. Not enough was done. The county court probation system failed this victim releasing Juliano Santana on three thousand dollars cash bail – thirty thousand surety bond. In all orders of protection, the perpetrator is required to forfeit all firearms. The fact that Juliano Santana had a firearm needs to be investigated. Did he have a license to carry the firearm he used in the killing? If so, this should have been taken away from him immediately upon the order by the judge on the day the victim went to police in Malden. Someone provided the gun, and someone knew that he had plans for using the weapon. The psychological autopsy can develop facts that shed light on these truths. The facts gleaned in the PA will directly help other cases like this one. The question always comes up as to how the guns were acquired or how the guns were not removed as mandated by law?
“The psychological autopsy is an individually designed case study that elicits a broad range of factual data regarding the behaviors of a decedent in the immediate day or days leading up to domestic violence homicide. The study is especially important when first responders and essential workers are involved. In all likelihood the girl lived in fear and terror” according to Michael Sefton, Ph.D. at a police psychology program in Worcester. This after incident examination can provide a good deal of information and warning signs that extreme risk for violence exists. These studies may add to the collective understanding of DVH – especially when family annihalation results.
We conducted a psychological autopsy on a man in Maine who murdered his wife and two children. This occurred just days before his divorce was to be finalized and two weeks before he was to be tried for criminal threatening. Steven Lake was known to be violent toward his wife and daughter. He violated the order of protection over five times with impunity. His firearms were not taken from him. He had over twenty to choose from when he made his move. This is what happens in systems where defense lawyer argues about eighth amendment rights to “reasonable” bail in lieu of consideration for the traumatized victim and her family. What modern society leaves its children at considerable risk for death in crimes like these? There were most certainly red flags that the perpetrator waved in the days and hours before this kidnapping and murder. His anger was likely extremely high as the trial date neared. He would not allow the victim to take control of his life by sending him to prison where he belonged.
Someone knew that this was going to happen and said nothing. Maybe a family member or co-worker. He may have contacted the victim wanting to apologize or threaten her against telling the truth. Or her family was threatened? But it is quite likely the unnamed 16-year-old lived in fear that her tormentor may strike and take her again. Just as he did on Thursday in late June as she walked to her home. It is vital to future cases of domestic violence that common red flags do not become holes in the safety plan of victims seeking safety and protection. The results of the psychological autopsy of Steven Lake were presented to the Maine Attorney General’s DV Homicide Review Board. The document is 75 pages long and offers over 50 recommendations for lowering risk and lowering deaths by DV.
Governor Charlie Baker had the right idea and proposed it to the legislature that allows the court to require a dangerousness evaluation in the case of rape and other crimes. We learned that this failed in 2022 as too expansive a mandate with too few resources to hold perpetrators accountable. Why? The Middlesex County D.A. should bring this to life and use the event to highlight the imbalance in domestic violence prosecution and the protections it gives to perpetrators from (low bail) and the fear it drowns its victims who feel unprotected. Even having an ankle monitor did not work until it was too late and provided no “real time” monitoring. If it had, then Santana could have been tracked when he diverted from his given route and came to Acton to murder his stepdaughter.
Everytown Research & Policy is a program of Everytown for Gun Safety Support Fund, an independent, non-partisan organization dedicated to understanding and reducing gun violence.
Career Burnout: The overwhelming impact of stress and understanding the cost to Human Capital
WESTBOROUGH, MA October 17, 2024 When we talk about career burn-out, we are looking at the impact of chronic and sometimes overwhelming stress on work efficiency and job satisfaction. As a clinical psychologist, I espouse the risk of stress and its associated malignancy to everyone I meet. Stress adds costs to workforce management because as workers become overwhelmed they start to look for better jobs. Surprisingly, it is often not the compensation that makes workers want to switch jobs – but the work ecology, those subtle factors most of us seek in the relationship between us and the company. Replacing intelligent and career oriented nurses and doctors is very expensive and disruptive to everyone. It means that supervisors are always interviewing and floor nurses are always orienting someone to the idiosyncrasies of the role.
It has been suggested that employees who are under chronic stress are at greater risk for making medical errors and other mistakes. Shortages in staff trickle down to patient care too. Hardly a day goes by when I do not hear someone say “I had to wait 30 minutes for someone to come and help me get back into bed.” When it comes to healthcare, people are not concerned with staff shortages when a loved one is hospitalized. Customer satisfaction is key to good medicine and community policing alike. And like police officers, a nurse or doctor who is on the last hours of a 12-hour shift is more likely to be ill-tempered and out of sorts. And like police officers, healthcare workers experience stress from long hours, shift work, and the nerver ending number of patients. Just ask any nurse or physician working in the emregency department and they will tell you it goes on and on round the clock. It is a mystery how some can stay in one job for any length of time given the current model of corporate medicine and the megagroup practice devouring one sole practitioner after another.
“The prolonged elevated cortisol levels that come with chronic stress and post-traumatic stress disorder (PTSD) can interfere with and damage the brain’s hippocampus” Wendy Suzuki author of Good Anxiety: Harnessing the Power of the Most Misunderstood Emotion.

The brain and body experience stress like a jolt of toxic hormones that have the power to gradually reduce the ability to relax and quiet the body. I am tasked with assessing employees following high acuity/high lethality calls for service who find themselves in an unsustainable state of physical tension and mental fatigue. I teach mindfullness and biofeedback strategies for people suffering with the effects of chronic exposure to high stress situations and the physical impact of these. When working with a group of medical providers stress may become overwhelming after a particularly stressful shift, like many hospitals experienced during the coronavirus pandemic.
I presented a conference on Stress and Healthcare providers: Caring for the Caregivers shortly after our emergence from the nationwide pandemic response in 2022. On that night, I wanted to bring some examples of current stress the frontline healthcare workers experience – especially with the pandemic now in the rear view mirror. In doing so I realized that even preparing for this 90 minute presentation was as much as I could handle with so much on my plate. I needed to remind myself, I am not a superman, I am not a warrior. I must take time for myself and cleanse my psyche of the evil spirits floating around in my unconscious mind. I am aware of the impact of stress on my thinking and my intimate life.
In the short term, our bodies need the adrenaline and cortisol to quickly activate our brains and other organs to react when a threat exists such as when a patient unexpectedly goes south. Since we were being chased my sabertooth tigers we have relied upon the “threat response” to keep us alive. In any environment our bodies need this fight-flight system to modulate and guide our behavior including when to run, fight, or freeze. It comes down to using our sensory system to be on guard for us and when we are exposed to something threatening, like a crash in our patient’s blood pressure or looking through a darkened building trying to find a burglar.
“If you exercise regularly, get good-quality sleep and take steps to reduce and/or manage your stress, “you can reduce stress activity in the brain, systemic inflammation and your risk of developing cardiovascular disease,” reported Ahmed Tawakol, a Massachusetts General Hospital physician quoted in Washington Post article on Stress published in 2022.
Chronic stress is hard on the human body. Most people who seek out a blog like this one are well aware of the toxic impact of an abnormal stress response. “The prolonged elevated cortisol levels that come with chronic stress and post-traumatic stress disorder (PTSD) can interfere with and damage the brain’s hippocampus, which is critical for long-term memory function,” Wendy Suzuki said in a Washinton Post article (2022). The hippocampus and amygdala are a constant filter for danger and threats to safety. Abnormal activation or damage to these organs leave a person struggling with constant activation of the fight-flight response that we know is unsustainable. Or even worse, we are left somewhat helpless without this cueing mechanism. When it starts to rain upon us and we do nothing to initiate staying dry or move away from the lightning. Long-term increases in cortisol can also damage the brain’s prefrontal cortex and its interconnective pathways. These are essential for focused attention and concentration, as well as the functioning of the higher order executive system needed for problem solving and other cognitive tasks we often take for granted. That is until they are corrupted by stress hormones running amock.
What are the signs of burnout? First, there are many nurses who have become numb and disinterested. Some career nurses pull the plug on their roles leaving to become a home health nurse or perhaps off to the nursing home nearest to their homes. Many experience caregiver fatigue and waning empathy from hours of high stress patient care and management. During the relentless pandemic Many want to go back to the “old way” of taking care of patients by using the primary nurse model which divides high acuity patient among the senior nurses on a shift. The primary nurse is usually repsonsible for attending team meetings designed to update physicians and consultants as to how treatment goals are being met.
Secondly, burnout can leave people exhausted, unmotivated, and cynical – the consequences of which can be catastrophic in many professions. As well as impacting professional growth, research suggests that these extreme stress levels can impair social skills, overwhelm cognitive ability, and eventually lead to changes in brain function and damaging physical disease and inflammation in vital organs leading to premature aging.
The stress of this is often overlooked. “During the pandemic began, newly minted residents who normally wouldn’t take care of patients with severe respiratory illnesses, such as those training to be psychiatrists, podiatrists, or orthopedic surgeons, have been asked to volunteer to work in COVID-19 wards” across the country according to a report by Deanna Pan in the Boston Globe on May 9, 2020. Professionals including residents in training, who ride a high stress career need time to process the trauma they face each day. That is not always possible. As a result, the cumulative impact can abbreviate even the most stalwart among us. Supportive supervision can assist young professionals to mitigate the impact of trauma and stress. Time for resilience should not be put off because of staffing shortages.
Working on the front lines with patients who are dying is horrific. This is especially painful when there is seemingly nothing that can be done to help them. First responders and frontline hospital workers are trained to provide emergency care. When their training is not effective, than feelings of helplessness will grow (Sefton, 2020). These feelings can be overwhelming. The cost has been great with increased rates of suicide since the shutdown began in March including those on the frontlines where the decisions they made both right and wrong may have been impacted by the unending stress of patient care.
On April 27, 2020 Lorna Breen, a physician specialist in emergency medicine took her own life after being witness to dozens of patient deaths during the peak of the coronavirus and contracting the virus herself and surviving it. Dr. Breen was a professional and emergency service medical director of NewYork-Presbyterian Allen Hospital and had no history of depression or mental health diagnoses.
More should be done for employees to assist them in remaining emotionally hardy and resilient for long-term career satisfaction. We know that days of stress from never ending patient flow can undermine career-oriented nurses and shorten their work life – something that no employer wants to see. The same as in law enforcement, finding replacements for nurses, doctors, and other caregivers is not easy. It is important to get ahead of career paths and lower the chances of losing the best and brightest because they are pushed too hard by a hallow system that does not care for its employees. Its human capital is the source of all business success. The loss of its human capital is the actual cost of stress and should be better addressed with thoughtful awareness, firm compassion, and kindness.
Stress awareness remains a key denominator for law enforcement for managing its malignant power to impair
WESTBOROUGH, MA September 23, 2023 – Police agencies across the country are looking for ways to mitigate the impact of accumulated stress associated with exposure to the worst of the worst of all human experience. These events happen everywhere and are unpredictable. “Arguably, everything from unattended death, domestic violence, child abuse, and a fatal motor vehicle crash can show up on the call board of any dispatcher on any day or night” according to Sefton, 2015. Career longevity and hardiness is essential for good law enforcement. There is a lot of training going on across the country emphasizing the importance of lowering stigma and bias against people with mental illness. Police officers and social workers are now found together in cars where mental illness is a suspected underpinning. The idea in not new and is known as jail diversion. For those with active mental illness diverting the citizen to behavioral healthcare is a better alternative than delivering them to the county holding facility. Programs for jail diversion are gradually making their way into small and medium sized departments across the country thanks to grants and political best practices. Gradually, the law enforcement field has had to look at itself and accept that when an officer is exposed to traumatic events over and over during his or her career, then we can expect that there will be an emotional response of some kind. That is a fact and impacts career longevity including physical and mental wellness.
Police officers are often hard charging men and women – especially right out of the academy and field training. They quickly go all in and no one wants to be seen as weak or unreliable. The field training is also being modified to allow officers to experience normal reactions to these early exposures. Things that can lead to stress and decreased efficiency as life circumstances change. Situations like marriage, children, buying a house, childcare, financial angst, you name it. Add to that mid-career professional jealousy and cynicism, career embitterment, resentment, staying current with court cases, mandatory overtime, holidays, and life becomes pretty hectic pretty quick. High stress situations require considerable time for all people to process. In law enforcement, time is something that is often a luxury. “Downtime is important for our health and our body, but also for our minds,” says Elissa Epel, M.D., a professor in the psychiatry department at the School of Medicine at the University of California at San Francisco. Some say that humans need 24 hours to process a high stress experience and return to normal balance.
“I have several posts that have brought up the human stress response going back to 2015 but there is plentiful research dating back 50 years or more on the human stress response and autonomic dysregulation. I believe strongly that unregulated sympathetic arousal can lead to a decline in physical well-being as the literature guides. The human cost of stress has been well studied and the effects of stress are a well-known cause of cardiovascular illness including heart attack and stroke and others. It is now known that the brain plays a big role in all of this.”
Stress is a cumulative response to exposure to threatening, fearful, or chaotic scenes. It is especially important that cops are able to quickly assess violent scenes to provide best and most timely action. Active shooter protocols require that teams of officers are not distracted in their search for the shooter sometimes stepping over victims along the way. It can become very difficult unless they are disciplined. “Officers are trained to be vigilant and alert. The job demands it. But these expectations, mixed with chronic exposure to stress can make officers hypervigilant and hyperalert even during moments of calm. The stress of police officers doesn’t suddenly disappear when a shift ends” as reported in Powerline on Law Enforcement, published in August 2023. Whenever I have participated in an after-incident review or formal defusing/debriefing, I rarely have an officer raise his or her hand when asked “did any of you experience significant stress during this call?” That is to be expected to some degree. But honest reporting on call-related stressors like an officer involved shooting, fatal car crash, sudden cardiac event in another officer, or domestic violence homicide should leave any one of us in an elevated state of stress. This comes from the brains response to fear producing events that all human beings experience and takes as long as 24 hours to return to normal. Some say police officers can be taught to reduce the effects of high stress call to 60 minutes. The problem with that is that many agencies with high call volume do not have the manpower to allow one of more officers to sit on the sideline as their stress response slowly trends down to normal. Men and women in law enforcement are vulnerable to chronic stress and many do nothing to mitigate this vulnerability.
For career hardiness it is essential that law enforcement officers manage their stress. This means regular exercise, a healthy diet, and stress awareness and mindful lowering the body’s elevated fight-flight response. Especially after exposure to the gut-wrenching calls that regularly come across the police scanner. Well-established research has shown that low-level daily stress can create such intense wear and tear on our body’s physiological systems that we see accelerated aging in our cells, says Elissa Epel, M.D. who co-wrote the book “The Telomere Effect.” Epel added: “Mindfulness-based interventions can slow biological aging by interrupting chronic stress, giving us freedom to deal with demanding situations without the wear and tear — and giving our bodies a break” as described in the Washington Post article authored by Jamie Serrano on June 29, 2024. In my experience, the techniques of mindfulness have an appreciable impact on lowering self-regulation described in most literature. The drawback is a lack of carryover and minimal positive practice. It is not for everybody but it can be one part of a comprehensive goal of self-care and emotional resilience needed for long-term career success. The importance of this practice cannot be overstated when cops frequently jump from one call to the next. I offer individual biofeedback sesssions to lower the body’s sympathetic activation that often ramp up at times of threat. For many in law enforcement, the experience of being under threat never goes away. This can hurt.
In the Spring of 2024, I was involved in a Zoom presentation on the important ways to unpack stress and its cumulative impact on physical and mental health offered by Whittier Rehabilitation Hospital in Westborough, MA. Like everything in the new year, innovative ideas and habits are hard to stick with. But building discipline is easier when one becomes committed to educated on what stress can do to our bodies and committed to using our skills to limit the daily accumulation of adrenaline and cortisol and recognizing the signs of an abnormal stress response. Things like poor sleep, irritability, excessive use of alcohol or drugs, forgetfulness, overeating, lack of exercise, isolation, etc. We all do these things at times, we are human. But when you find yourself going off the rails, and are not taking proper care of yourself, it may be a sign of a growing stress response that may lead to depression, anxiety, and a host of physical conditions like hypertension, heart disease, stroke, autoimmune disorders, obesity, and diabetes. A balance of work and personal life should be part of any stress lowering plan. It becomes especially important to pull yourself back into your routine. Things like exercise, nutrition, mindfulness lowering alcohol intake, regular sleep, and maintaining family and social connections become key tasks to help you feel better and lower shame and guilt.
“If we perceive our available resources to be insufficient, along comes the ‘threat’ mindset. When threatened, stress has a catastrophic effect on our ability to perform. We receive an enormous sympathetic surge (adrenaline/noradrenaline dump), and our HPA axis pumps out cortisol. High cortisol levels have a very detrimental effect on higher cognitive processes – decision-making and prioritization” as described in a blog written by Robert Lloyd, MD.
I conduct pre-employment psychological screening here in Massachusetts. Men and women entering the field today are smart and well-educated. Academy curricula integrate behavioral health and officer well-being more than ever teaching students to utilize stress response strategies to lower the threat response sometimes aberrant in acute stress reactions. Agencies like the RCMP and the Finnish Elite Police service are using paced breathing techniques to quickly reduce the effects of high adrenaline that is a hindrance to physical and cognitive functioning. These techniques are easily taught and when learned, need little to no technology or equipment to implement.
According to Leo Polizoti, Ph.D., the primary author of the Police Chief’s Guide to Mental Illness and Mental Health Emergencies, and colleague, stress can lead to a breakdown in adaptive coping. “Learned resilience can be taught and leads to reduced stress and psychological hardiness rather than psychological weariness and burnout. Psychological weariness is a drain on coping skill and regular adaptation to job-related stress needed for efficiency for handling the everyday calls for service. Resilience and career satisfaction are important components of law enforcement and individual officer training, on-duty behavior, and career longevity. Positive resilience will reduce officer burnout, misconduct, and reduce civilian complaints against officers.
Some law enforcement officer deaths may be reduced by using a stress intervention continuum as a way to get out ahead of the buildup of stress. This program ties the range of calls into a stress reduction protocol that empowers resilience and recognizes the importance of stress mentoring and the soft hand-off for defusing the growing impact of high stress and high lethality exposure. If 10 cars are sent to a fatal automobile accident with entrapment, then these officers would be expected to participate in an after-action defusing of the incident. Those 10 units would also be coded with a level 1 call – highest level of acuity. This is easy technology and cars are often dispatched to level 1, 2, or 3 depending upon the severity of the call. It becomes an end-of-the-year task to see which officers have accumulated the highest number of Level 1 high acuity calls. Level 1 is highest priority and puts the officer at highest risk for exposure to traumatic stress and its debilitating impact.
The stress intervention continuum does not single out one officer but identifies all officers – including call takers, dispatchers, and supervisors for defusing particularly abhorrent events like mass shootings, domestic violence homicide, or fatal car crashes. This way, personnel who played a roll in a “bad call” will not be overlooked nor stigmatized for stress reduction defusing and/or debriefing. Chief Paul Saucier who is the interim chief of police in Worcester MA requires that officers attend a post incident defusing after major events with high lethality or particularly lurid stressors. Worcester PD is an agency with over 400 officers and may participate in this program. More agencies are beginning to utilize some form of online screening that officers may complete on an annual basis that measures perceived stress over the previous month. Chief Saucier and I have discussed options for on-line assessment and annual reviews. I have looked at the Perceived Stress Scale – PSS-10 for implementation.
LODD – Unsustainable pain in the thin blue line

I recently read an article in the Washington Post first published in 2018 written by Michael Miller. I sent him a note suggesting he pick up the ball on this. I am interested in the topic of police behavioral health and understand the dynamic of law enforcement suicide and how the notion remains stuck in modern police service due to stigma with suicide and mental health wellness in police officers. I am a former police officer and know there is nothing more horrific than a police officer suicide or death to a member. In Chicago officers have taken their own lives while in the driveway of their duty station. In Los Angeles, four active duty or retired officers committed suicide in one weekend in November 2023. In Washington DC, an officer who was ordered back to work following the attack on the Capitol killed himself while driving to his work. People are starting to connect years of service with risk for suicide and many departments are taking police officer wellness as the key to both career hardiness and job performance. One officer granted LODD status remains in conflict. Erin Smith wants her husband’s name added to the D.C. police department’s list of fallen officers and engraved on the National Law Enforcement Officers Memorial, and the official burial honors traditionally afforded to officers killed in the line of duty according to a Washington Post opinion piece from .
I was part of a panel about police suicide in Chicago in 2019. The dark problem is especially taboo when cops are involved in a line of duty shooting and later kill themselves. The Chicago program was held following a rash of suicide deaths in the Chicago PD. Most officers do not return to the job following the investigation of their actions. Some do. Those who do return are off the job within five years. I am a police consulting psychologist in the Boston area. I am charged with pre-employment screening and fitness for duty exams after law enforcement exposure to trauma. More needs to be done to link on-the-job exposure to horrific and despicable human behavior to suicide and afford them line of duty death status including the honors and pension compensation just like other officers who die in the line of duty. In Washington DC officers who took their own lives following the Capitol insurrection were afforded line of duty status. Why not others?
“Police work took officers to “some of the darkest places in America,” he said, and few were darker than the scenes of officer-involved shootings, often called “critical incidents.” Line of duty death and police well-being are strongly impacted. Some police officers kill themselves after critical incidents they cannot unsee.”
“Chicago is kind of like ground zero with the number of suicides that are happening on a monthly basis now at this point,” said Daniel Hollar, who chairs the department of behavior and social science studies at Bethune-Cookman University in Florida. Dr Holler hosted Dr Doug Joiner to Chicago for a symposium in 2019. Dr Joiner taught us much of why officers kill themselves. He says they become embittered, they feel a deep sense of thwarted belongingness and grow increasingly detached with higher risk of suicide. “These are police officers answering calls of duty to protect lives. We (need to) do our job to make their jobs safer.” said Dr. Joiner. After an officer suicide, personnel try to reconstruct what was going on in the person’s mind by systematically asking a set of questions, in a consistent format, to the people with the greatest insights into the person’s life and mind—family, co-workers, and friends.” This is known as a psychological autopsy, and I have proposed it for any officer who dies by suicide. If this is done effectively, I can assure you there will be no escalation of suicide among police officers. Something police chiefs and city counselors unfairly fear.
I am working with one department where two officers have not returned to active duty nearly two years after being involved in a violent shooting while trying to help someone who had led them on a chase ending in a roll over motor vehicle crash. As officers approach the overturned vehicle the driver began shooting at them with a semiautomatic rifle. These brave men were traumatized by the fatal shooting of a subject who first fled from a legal police car stop and then opened fire on them. They have been out of work on administrative leave receiving behavioral health support but are unlikely to return to service.
I have conducted a psychological autopsy on a police constable who was involved in a line of duty shooting resulting in death in November 1971. He was a full-time police officer in Mifflin Township, OH that had no formal police department. No chief and no field training support. He shot and killed a man and was cleared of wrongdoing. Sadly, he killed himself in front of his wife one year later at Christmas. He grew restless and embittered after being villified by people inhis community. He believed nothing was being done to support and protect him. He is buried in a cemetery near the man he shot and killed. I want this death changed to line of duty (LODD). Why? When someone kills themselves most departments, including all smaller agencies, fail to discover the set of facts and red flags left behind leading to suicide. The investigation is often cursory, purportedly out of respect to the family. But there are factors in the careers of police officers that make them at higher risk for suicide then the public. This is not sustainable.
I have been writing about this for 9 years in the pages of my human behavior blog. In Chicago, if an officer comes forward looking for help, they are stripped of their firearm, police powers, and their star (badge). This is demoralizing according to officers I have spoken to. Why would anyone come forward if this is the protocol. This may be changing, whereas CPD has added therapists in each of their 23 police stations. Unfortunately, one cannot unsee some of the darkest scenes in human behavior like the death of a law enforcement officer or domestic violence resulting in death. The psychological autopsy must include a 3-month list of calls the decedent answered including those for which he or she was given debriefing, defusing, or time off for respite from the job. I would want to understand how the call volume may have triggered underlying acute stress of new calls that triggered new trauma? In any case, the story was interesting and careful analysis is important in all incidents resulting in police suicide.
Writing reports that work for victims of DV: Tools for measuring risk for DVH
There were times that at the end of a midnight shift in Westbrook, Maine, outside Portland, and New Braintree PD, in Massachusetts that I had reports to write for incidents I had been assigned during the shift. More than once, I snuck out of the patrol office and went home – too tired to write. And more then once, the sleep I so wanted was disturbed by the day sergeant or court officer looking for my report. Or sometimes, when I did stay, my writing was not my best effort because I was tired. Report writing is an art and is now a large part of both the academy training and field training programs. Law enforcement officers are better trained and more highly educated than ever which is essential in these times where every word is public property. The media, the citizenry, and the police hierarchy are all slicing and dicing every paragraph of today’s reports looking for your mistakes, it seems. The reason I write this is that police reports have consequences and if important statements, or officer observations, or photographs are omitted, cases may be lost. It is essential that report writing be taken seriously because, in the setting of domestic violence, lives depend on it.
Just like any report document that is to be handed out to anyone who might request it, particularly underpaid defense attorneys who swim in circles, like sharks looking to devour a poorly written report and its author. Report writing needs to be concise and laser focused. Particularly important is the reason for the call. Why did this victim call today? We know that the abuse tends to escalate successively. Sometimes, it is only when children become involved that a victim will move to stop the violence. In Vermont, a teen boy shot and killed his father when the man drunkenly waved a pistol threatening the family. And in Maine, a 13 year old boy was found to be hiding a 20 gauge shotgun and ammunition on the day he and his family were murdered by his father Steven Lake. Our analysis of the Maine case led us to understand that the boy was likely intending to defend his mother and sister against a violent and unpredictable father. He may have been seeking to load the weapon when his father snuck into the unlocked house and overpowered the family. 20 gauge shells were found in the child’s bed and under his pillow.

When conducting assessments or forensic exams with a victim of domestic violence (DV), any reported history of strangulation places the person at a higher risk for more serious violence or homicide by the hands of their intimate partner. By recognizing signs of strangulation, healthcare providers can help to mitigate long-term damage, properly document any evidence of abuse, and provide referrals for seeking safety assistance. Sara Vehling 2019
Risk assessment tools provide quantifiable data that may be used to develop actuarial projections as to degree of risk and dangerousness. Report writing now should include assessment tools that uncover potential risk to victims. Jacqueline Campbell, RN has a valid risk assessment tool for determining whether there is high risk to potential victims that can be living in the home while officers are still on scene. Campbell’s work is readily available in the DV literature and known to most of us. The Ontario group in Canada also has a reliable tool – ODARA used by law enforcement agencies across the country. In my agency we adopted both tools after the research was complete from The Maine homicides. The national leadership includes Lenore Walker, in addition to Campbell, who both have published a good deal over 25 years on DV and its cycle. Walker believes that women and families are exposed to great harm when the abuser is out of jail only hours after terrorizing his family. It rarely mitigated the next beating.
I propose holding the abuser until his first arraignment perhaps as long as 2 days. This allows for a cooling off period. Minutes are like hours while sitting in a municipal cell block often eating fast food 3 times a day. But the 8th Amendment of the Constitution guarantees that bail shall not be unfairly denied or excessively harsh. In truth, the modification of bail conditions in some instances must be done in real time to account for the severity of individual cases of DV and unique red flags. Experts have said that when a victims says ”I know he is going to kill me” then there is a greater likelihood that she may be correct and a protective, safety plan should be put in place. On the continuum of risk, expecting to be killed is only slightly less dangerous as physical attempt to kill or maim. In these most dangerous cases, there are tactical measures that must be written into protective orders such as GPS monitoring, forfeited bail and remand to custody for violation of protective orders, social media restriction, no contact with victim and children, no contact with victim’s family or friends, and supervised visitation, when only appropriate. It is these cases where the police officer’s report must be first rate and bullet proof.
A period of being held in custody until initial arraignment will enhance public safety and public trust in the short run. If applied to all persons arrested because of domestic abuse, then it would not unfairly impact only the poor or disenfranchised. Abuser’s should not be able to buy their way out of jail nor should they be free to wander their communities stalking their supposed loved ones. Steven Lake who killed his family and himself in Dexter, Maine posted his love for his children nightly and had piteous social media “friends” encouraging him to “fight for his children”. Little did they know he was planning the onerous events that would end the Lake family timeline forever. The Maine Law Review in 2012 reviewed changes in conditions of bail and cited our research over 12 times in its review of conditions for the release of persons in jail for domestic violence. Protective factors include the abuser having full employment and a substance free environment.
As the reader begins to understand report writing requires a visceral response and poignant understanding of this hidden social maelstrom. There are legitimate reasons for seeking “no bail” holds on some people arrested for domestic violence when high acuity and high risk exist together. These have been posted by me in the Human Behavior blog.
Campbell, J. (1995). Assessing dangerousness. Newbury Park: Sage. Nicole R.
Bissonnette, Domestic Violence and Enforcement of Protection from Abuse Orders: Simple Fixes to Help Prevent Intra-Family Homicide, 65 Me. L. Rev. 287 (2012). Available at: https://digitalcommons.mainelaw.maine.edu/mlr/vol65/iss1/12
Ronald Allanach et al. (2011) Psychological Autopsy of June 13, 2011, Dexter, Maine Domestic Violence Homicides and Suicide: Final Report 39 (Nov. 28, 2011), http://pinetreewatchdog.org/files/2011/12/Dexter-DVH-Psychological-Autopsy-Final-Report-112811-111.pdf.
Vehling, S. (2019) Taking your breath away – why strangulation in domestic violence is a huge red flag. Blog post https://www.mobileodt.com/blog/taking-your-breath-away-why-strangulation-in-domestic-violence-is-a-huge-red-flag/ taken March 15, 2022
Mac Walton. (2019) Bail Reform and Intimate Partner Violence in Maine, 71 Me. L. Rev. 139. Available at: https://digitalcommons.mainelaw.maine.edu/mlr/vol71/iss1/62
Get rid of stigma once and for all
This video is about an introduction to a post that will be forthcoming in a short while it is reference to law enforcement officers and the suicide death of officers who carry trauma.
The NYPD is making use of psychological autopsies, a research-based approach that attempts to better understand why someone took his or her life.
The fight/flight mechanism that keeps us on guard plays a primary role on how people feel after episodes of high stress. Feelings of frustration, lack of focus, chronic fatigue, and even depression can result from an over reliance social media stimuli like an unfed addiction.
Loneliness, loss, and fading resilience in the tarnished golden years: languishing with loss of purpose
 The isolation felt by people in quarantine can leave the average person feeling numb and emotionally languished. Recently, I provided a zoom conference on the psychological impact of the coronavirus in November 2021 from my office at Whittier Rehabilitation Hospital in Westborough, MA. It was well attended, largely by people who are psychologically minded and aware of the points I endeavored to make. My target audience was the people who were struggling and vulnerable to decreased coping during covid-19 recovery. I am unsure we hit the mark I was hoping for with the target audience.
The fallout in mental health from the coronavirus is real and it is now recognized as a public health menace among recovering adults. It is now being seen in children and adolescents with growing concern. Just like younger patients, loneliness and social isolation in older Americans are serious public health concerns putting them at risk for dementia and other serious health conditions including failure to thrive, sepsis, malnutrition, addiction, and mental illness according to a CDC report. For many individuals in quarantine, the nightly happy hour started earlier and earlier raising the specter of worsening substance abuse and addiction. The liquor stores were soon to be considered essential services and package delivery became a common source of re-supply.
The impact of isolation, emotional loss, and social detachment undermines public and behavioral well-being across the life span. It is a co-occuring illness among illnesses afflicting millions. I see it in my own family as nerves are frayed now almost 2 years in – first noted in the blog post published in May, 2020 (Sefton, M.). In this fourth wave of the virus called the Omicron variant, people are tired of hearing about social distancing, mask mandates, and rising infection numbers. I see it every day.
The isolation felt by people in quarantine can leave the average person feeling numb and emotionally languished. Recently, I provided a zoom conference on the psychological impact of the coronavirus in November 2021 from my office at Whittier Rehabilitation Hospital in Westborough, MA. It was well attended, largely by people who are psychologically minded and aware of the points I endeavored to make. My target audience was the people who were struggling and vulnerable to decreased coping during covid-19 recovery. I am unsure we hit the mark I was hoping for with the target audience.
The fallout in mental health from the coronavirus is real and it is now recognized as a public health menace among recovering adults. It is now being seen in children and adolescents with growing concern. Just like younger patients, loneliness and social isolation in older Americans are serious public health concerns putting them at risk for dementia and other serious health conditions including failure to thrive, sepsis, malnutrition, addiction, and mental illness according to a CDC report. For many individuals in quarantine, the nightly happy hour started earlier and earlier raising the specter of worsening substance abuse and addiction. The liquor stores were soon to be considered essential services and package delivery became a common source of re-supply.
The impact of isolation, emotional loss, and social detachment undermines public and behavioral well-being across the life span. It is a co-occuring illness among illnesses afflicting millions. I see it in my own family as nerves are frayed now almost 2 years in – first noted in the blog post published in May, 2020 (Sefton, M.). In this fourth wave of the virus called the Omicron variant, people are tired of hearing about social distancing, mask mandates, and rising infection numbers. I see it every day.
 I have worked with older clients for over 25 years first as a post doctoral fellow at Boston City Hospital – now BUMC. Long before the pandemic, my work at Whittier Rehabilitation Hospital has been to provide support and direct service to patients’ suffering from debility associated with decline in physical health along with the psychosocial needs and changes. All too often, this includes feelings of loss of control and sadness that is palpable in our short conversations. Many seniors feel invisible and the virus exacerbates these feelings. Declining health further instills the loss of purpose and amplifies the stigma of being seemingly infirm. The lack of purpose germinates from the passing of a spouse, close friends who move or have died, food and financial insecurity. It precedes a death wish and it’s associated demoralization. My mother was infected with the coronavirus in mid-April 2020 before the vaccine was introduced. She lived in the same nursing facility where I lost my 93-year old aunt in the first wave of the virus in May, 2020. My mother survived the virus but it has taken a significant toll on her physical and cognitive well-being. We were not permitted to see my mother during her illness and my aunt was alone on May 1 when she succumbed to the virus.
I have worked with older clients for over 25 years first as a post doctoral fellow at Boston City Hospital – now BUMC. Long before the pandemic, my work at Whittier Rehabilitation Hospital has been to provide support and direct service to patients’ suffering from debility associated with decline in physical health along with the psychosocial needs and changes. All too often, this includes feelings of loss of control and sadness that is palpable in our short conversations. Many seniors feel invisible and the virus exacerbates these feelings. Declining health further instills the loss of purpose and amplifies the stigma of being seemingly infirm. The lack of purpose germinates from the passing of a spouse, close friends who move or have died, food and financial insecurity. It precedes a death wish and it’s associated demoralization. My mother was infected with the coronavirus in mid-April 2020 before the vaccine was introduced. She lived in the same nursing facility where I lost my 93-year old aunt in the first wave of the virus in May, 2020. My mother survived the virus but it has taken a significant toll on her physical and cognitive well-being. We were not permitted to see my mother during her illness and my aunt was alone on May 1 when she succumbed to the virus.
Trauma informed therapy refers to the critical understanding of one’s emotional history and supports the model of early traumatic experience being one underpinning of many mental health outcomes and threatened resilience later in life. These kinds of experiences have an impact on people who have had loved ones die while in lock down across the country and can engender guilt and helplessness. Often, singular front line medical staff are alone with patients who succumbed to the virus – sometimes holding the fading grip of another disappearing life. This heroic act of empathy happens without fanfare or even a moment to process its importance and acknowledgment of the person’s passing.
Hurry up: you are called to help save lives but are told to do nothing!
The man stopped breathing.His color signaled that he had only moments to live. His nurse called the code. This brought a hospital team of

nearly 20 staff members assigned to the code blue team. Their job was to provide intervention for advanced cardiac care to return circulation and restore breathing. Every member of this team had a job to do. Starting with the scribe who kept track of everything. “Is somebody writing”? Inquired the maestro. Things like the minutes since the heart stopped and when he first received medication, when IV access was achieved, or the time he received the lifesaving shock to his heart, known as defibrillation. Her voice was sometimes shrill as she tried in vain to speak above the calamitous scene by tracking time since last dose of epinephrine, adenosine, or vasopressin or changing vital signs. Her job was essential and had to be accurate. These are high stress low frequency events that nobody enjoys.
The code team works like an orchestra led by the maestro – sometimes a senior nurse. The maestro must be laser focused and have full knowledge of the patient’s recent medical history and all possible causes leading to this event. Maestro follows an ACLS protocol that guides the decision tree. The team had assigned jobs for CPR and back-up to the person assigned to be first on chest compressions. And there was the rescue breather, respiratory therapist, IV nurse, the runner for blood and other equipment, pharmacist, and physician – usually the maestro. For many team members, there is an intangible calling that underlies a doting sense of purpose which brings them into nursing.The less experienced team members may be second chair in this orchestra but all feel cheated when outcomes are bad.
The man in question wanted no heroic measures taken and did not wish to be transferred to the trauma center if his heart were to stop beating. It was his advanced directive.
On this particular day, the nursing staff on duty watched the patient closely. His heart was being monitored for rate and rhythm. His breathing sounded scary in the early morning hours on the Saturday after Thanksgiving. The family had not been able to see the man who had been diagnosed with covid-19 following a stroke. By all reports his viral load was mild. He seemed to be getting better leaving most of us to believe he would slowly improve and one day make it home. I spent time with him that Friday assessing his language. It too had improved during his time in the unit.
The physician on the day shift was not on the unit yet on the Saturday morning. It would be the man’s last day. He was running a low grade fever perhaps 99.8 degrees. This was lower than it had been the days prior. The man had started to show signs of improvement after being diagnosed with coronavirus shortly after being admitted to the rehabilitation hospital. He was fully vaccinated. So what happened? He went from being on the mend to not breathing in a matter of hours. This is what front line ICU nurses and doctors have been dealing with for 18 months during this pandemic. We saw very few cases of this type at our hospital. Afterall, he was in our hospital to rehab from his CVA.
These events take a human toll and put a chink in the armour. Outcomes whittle away at job satisfaction, personal efficacy, and professional.purpose. The coronavirus was making its fourth appearance with a growing wave of breakthrough cases which had us all on edge. The man in this case was sick well before my breakthrough surprise. I became infected in mid-December and was sent home for quarantine.
The man was transferred to us following a significant left hemisphere stroke. He was sent for retraining to advance the functionality of his language so he might return home. He had global aphasia but was getting better with using words and helping himself. Slowly, his receptive language was starting to make connections again. He started to understand nuance and gesture. He could make his point using the tools he was learning during therapy sessions. These are good signs in early stroke recovery and represent the plasticity in the human brain. He had become able to follow some perfunctory directions and express his basic needs, still sometimes missing the point by using jargon. This is known as the language of confusion in speech pathology circles. We have excellent speech pathology services at Whittier and I especially respect their efforts and expertise.
He was not depressed and was working with his therapy team as much as he could. For their part, the staff is passionate when it comes to helping patients gain function. By standing, speaking, and eventually, directing their own care.
When he was admitted, the man and his family decided that they wanted no heroic measures taken should his heart stop beating. No CPR, no intubation or breathing tube, no transport to a higher level of care such as the nearby trauma center. He was not a young man and believed he had lived a good life. His wishes.
Remember, his breathing and respiratory drive took a rapid turn for the worse. Quickly, he went from looking bad to looking better, to looking worse. In a matter of a few hours his breathing had become more shallow. Agonal in quality. His nurse called the code.
Agonal breathing usually signals a cardiac arrest. Nurses are trained to respond with the code cart and a dozen or more advanced cardiac rescue interventions geared toward restarting the heart and saving a life. Not the outcome last Saturday morning. His choice was very clear – no heroic measures. So staff were instructed to stand down and watch. Some staff became emotional and were consoled by senior nurses.They could do nothing but sit on their hands.
The younger staff felt traumatized, as this was not supposed to happen. Even support personnel were watching as team members slowly backed away to hear witness.
His family was called and the sad news was shared. They had not said goodbye because of the mandated virus protocols. He did not yet receive the Sacrament of the Sick, as he had wanted. He was not alone and in the end, the group came together to recognize this man for the good fight he brought forth at rehab and for having the courage to know what he did not want, and for those few things he did. He died at 8:12 as he wished, without fanfare. The maestro on this day, reminded them all of this and that he lived a full life, and the scribe recorded the time.
“Long haul cognitive effects of Covid-19” in those who have “recovered”
There are now sufficient numbers of individuals who have had the coronavirus during the past 15 months who are presenting to their physicians with lingering symptoms of the disease. They are now known as long-haulers. People who have sometimes multiple complaints that suggest to researchers that they are a different group of patients. They tend to be younger, they generally have more complex medical histories including a variety to pulmonary conditions, and they are not the case you might expect to be most debilitated. This report is derived from the literature recent review and live zoom presentation on the Cognitive Impact on Long-haul survivors of the coronavirus held on May 20, 2021. It is available on the Whittier Health website. I want to thank Lauren Guenon, MS, SLP, CBIS for her help in this program and the data mining we are continuing.

It was first reported that overwhelming viral spread was thought to be primarily respiratory. The virus multiplies inside the body and is likely to cause mild symptoms that may be confused with a common cold or flu. This changes in many as the viral load evokes a cytokine autoimmune response in the body. As the virus takes, hold during the worsening pulmonary phase primarily respiratory symptoms such as persistent cough, shortness of breath, and low oxygen levels are observed. Too many survivors say the ignored this phase and just tried to rest at home. Often they were transported to hospital after being overwhelmed by the inflammation in their lungs and other organs. Hyperinflammatory phase, occurs when a hyperactivated immune system may cause injury to the heart, kidneys, and other organs as covid-19 devours healthy cells leading to death of cells in a process called apotosis.
Experience shows most long-haulers were expected to fall into the high risk category. like those with chronic COPD, but there is also a growing percentage of people who were otherwise healthy before they became infected and are not the older, sicker cases first described.
About 33% of COVID-19 patients who were never sick enough to require hospitalization continue to complain months later of symptoms like fatigue, loss of smell or taste and “brain fog,” that can interfere with functional tasks including the return to work.
University of Washington (UW)
It remains unclear if neurological complications are due to the direct viral infection of the nervous system, or they are a consequence of the immune reaction against the virus in patients who presented pre-existing deficits or had a certain detrimental immune response from their immunocompromised status when infected. 38 males, ages 22-74
The first studies of long haul survivors are being published. They are small studies reporting on the Italian first wave in 2020. The cases are hospitalized, non-intensive COVID units in Milan, Italy. These were not the patients who needed intubation or ventilatory support. Most had ARDS (mild, moderate, severe) Ferrucci, R et al. Subjectively, 31.6% reported overall cognitive decline 4-5 months after discharge when they were screened using a commonly administered cognitive test, then assessed using BRB-NT. Results for this group of moderately infected patients included: 42.1% processing speed deficits; 26.3% delayed verbal recall; 10.5% immediate verbal recall; 18.4% impaired visual long term memory, 15.8% visual short term memory; and 7.9% semantic verbal fluency deficits. Helms et al. reported on 58 patients who were evaluated in the ICU with over a third (33%) exhibiting dysexecutive syndrome, poorly deployed attention, and decreased capacity for organization
In another Italian study, 81% of patients had cognitive deficits including difficulty in areas of attention and executive functioning with pronounced weaknesses in divided and sustained attention (complex attention) set-shifting, speed of processing, and working memory. This was a group of 57 patients who were sent to acute rehabilitation after they were cleared of having active virus. All were debilitated and had a mean age of 64. 75 percent were male, 61 percent non-white and 56 percent were fully employed. In this group 88 % had suffered hypoxic respiratory failure with most being intubated for ventilatory support. 29% went on to get a tracheostomy tube inserted indicating a likely longer-term need for breathing support. 84 % need assistance with activities of daily living, has impaired mobility, and support for IADL’s. Neuropsychology services saw them an average 6.6 days after admission to the rehabilitation hospital. In general, the Whittier cases admitted for covid-recovery were referred to a neuropsychologist within 48 hours of admission. Ventilation-induced hypercapnia has been experimentally shown to lead to cognitive impairment due to acute inflammatory response advancing the cytokine storm and its multi-system impact.
Studies have described long-term risk and short-term risk to cognitive health from the coronavirus. Severe cognitive decline like dementia may be associated with co-occurring illness from anoxia, respiratory failure, blood clots and is associated with more severe disease and chronic long lasting symptoms. These are linked to prolonged risk of systemic inflammatory illness, increased risk of stroke and white matter disease within the brain and even reported cases of acute transverse myelitis (Budson,A, 2021). Budson reported on symptoms in 30-50 percent of people who experienced mild to moderate disease. Zhou et al. described a sample of 29 patients who were assessed 3 weeks after discharge home who were found to have dysfunction in the system of attention – most notably in sustained attention and reaction time. This may be the result of decreased mental endurance, slow processing and fatigue that are reported across several studies reported here. These patients were positively coorlated with C-reactive protein – a marker of the bodies inflammatory response when elevated.
Elevated level of CRP may be a valuable early marker in predicting the possibility of disease progression in non‐severe patients with COVID‐19, which can help health workers to identify those patients an early stage for early treatment.
Nurshad, A 2020
Rampage published in the table below in the American Journal of Speech Pathology in 2020. The long-haul covid-recovered are likened to patients described as having post-intensive care syndrome that occurs as a result of the changes in the system of cognition and emotional regulation. This is one of the best tables I have seen that illustrates the impact of the virus and the systems that are impacted. Rampage et al.
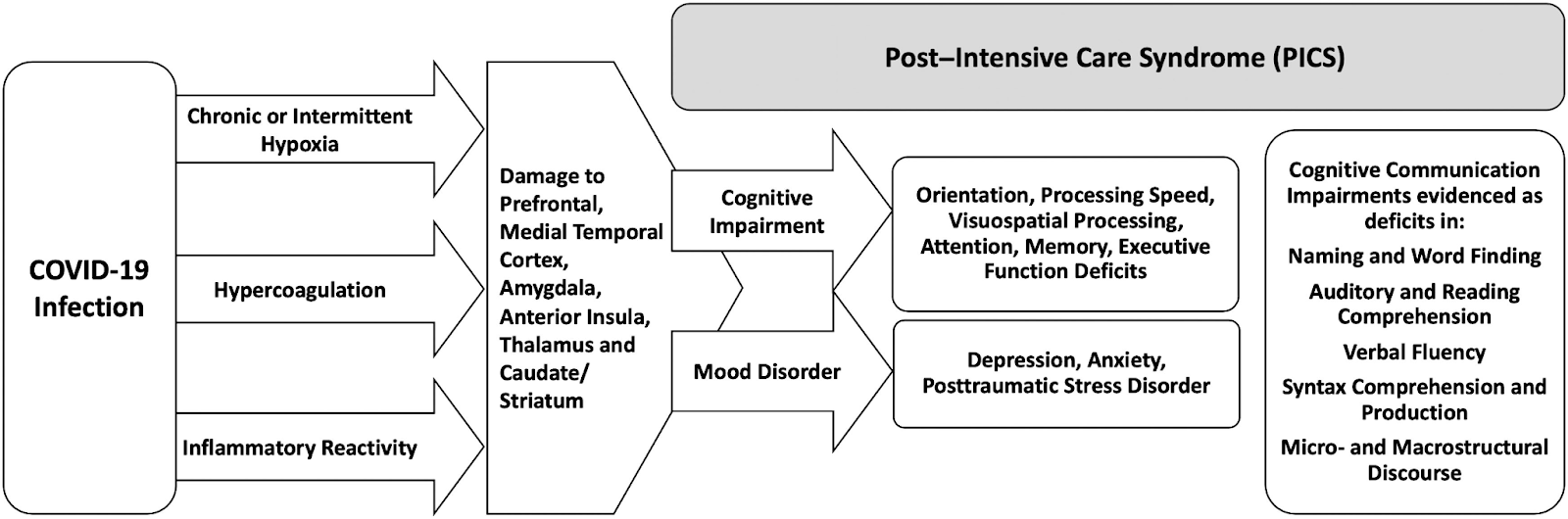
Delirium is another concern and fits in with what is called post-ICU syndrome (PICS), a collection of problems that can present—and linger—after a critical illness. “The three domains we worry about are impairments in physical function, cognitive function, and mental health” .
Yale School of Medicine Carrie MacMillen June 2020
The long term impact may be seen later on in life. Chronic systemic inflammation has been shown to promote cognitive decline and neurodegenerative disease makes it more likely that COVID-19 survivors will experience neurodegeneration in later years that has been known for a long time. Those with short term cognitive consequences may have had less viral load and for a shorter duration of time. Interestingly, those who were in covid-recovery units and on ventilators tended to report less cognitive symptoms suggesting there may have been some protective element to consistent ventilatory or simply timing and getting to the hospital before the hyperinflammatory (cytokine storm) phase of the viral process. A global increase in the prevalence of fatigue, brain fog, depression and other “sickness behavior”-like symptoms implicates a possible dysregulation in neuroimmune mechanisms even among those never infected by the virus .
Whittier Rehabilitation Hospital in Westborough, MA is looking at the data of 73 patients. This is very likely the first and largest subset of surviving long haul cases of the coronavirus. Our population is older 70.6 years, 66% white males versus approximately 64 years reported in the Italian studies reported here. The Italian samples were largely male as well. The average length of stay was 19.6 days. 21% had signs and symptoms of clinical depression or generalized anxiety co-occurring with their physical and cognitive symptoms. 14% had persistent delirium and encephalopathy.
Recovery from the long-haul symptoms reported in this paper will take weeks to months we predict. It has been recommended that aggressive multidisciplinary rehabilitation be initiated as soon as endurance permits. Intensity shoould include 4-5 times a week PT, OT, and speech language pathology. In many cases the comorbid depression and anxiety must be dealt with concurrent to the restorative physical and cognitive work. Some have likened the neurocognitive impact of covid-19 to that of a moderate traumatic brain injury in the breadth of its impact and tough return to a semblance of normalcy. Aggressive treatment is strongly recommended and should be commensurate with endurance and debility. There is evidence that the likelihood of full return to work is decreased after 6 months or more of recovery.
References
Ferrucci, R et al., (2021) Brain Sci. 11, 235.
Jaywant et al., (2021) Neuropsychopharmacology, 0:1-6
Budson, A. (2021) B.U.Medical School — https://www.health.harvard.edu/blog/author/abudson
Heneka et al. (2020) Alzheimer’s Research & Therapy. Long and Short-term Cognitive Impact of Coronavirus. 12:69 https://doi.org/10.1186/s13195-020-00640-3
Lawton, MP, Brody, EM. (1969). Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 9(3): 179-186.
Ramage, A. Potential for Cognitive Communication Impairment in COVID-19 Survivors: A Call to Action for Speech Language Pathologists. Nov. 2020, American Journal of Speech-Language Pathology. Vol. 29. 1821-1832
Sigurvinsdottir, R, Thorisdottir, I, Gylfason, HF. (2020). The Impact of Covid-19 on Mental Health: The role of Locus of Control and Internet Use. International Journal of Environmental Research and Public Health, 17:6985: doi:10.3390/ijerph17196985.
Nurshad, Ali, (2020) J Med Virol. Jun 9 : 10.1002/jmv.26097.
Ludovica Brusaferri, Zeynab Alshelh, Daniel Martins, Minhae Kim, Akila Weerasekera, Hope Housman, Erin J. Morrissey, Paulina C. Knight, Kelly A. Castro-Blanco, Daniel S. Albrecht, Chieh-En Tseng, Nicole R. Zürcher, Eva-Maria Ratai, Oluwaseun Akeju, Meena M. Makary, Ciprian Catana, Nathaniel D. Mercaldo, Nouchine Hadjikhani, Mattia Veronese, Federico Turkheimer, Bruce R. Rosen, Jacob M. Hooker, Marco L. Loggia (2022) The pandemic brain: Neuroinflammation in non-infected individuals during the COVID-19 pandemic, Brain, Behavior, and Immunity, Volume 102, Pages 89-97, ISSN 0889-1591, https://doi.org/10.1016/j.bbi.2022.02.018.
