WESTBOROUGH, MA October 17, 2024 When we talk about career burn-out, we are looking at the impact of chronic and sometimes overwhelming stress on work efficiency and job satisfaction. As a clinical psychologist, I espouse the risk of stress and its associated malignancy to everyone I meet. Stress adds costs to workforce management because as workers become overwhelmed they start to look for better jobs. Surprisingly, it is often not the compensation that makes workers want to switch jobs – but the work ecology, those subtle factors most of us seek in the relationship between us and the company. Replacing intelligent and career oriented nurses and doctors is very expensive and disruptive to everyone. It means that supervisors are always interviewing and floor nurses are always orienting someone to the idiosyncrasies of the role.
It has been suggested that employees who are under chronic stress are at greater risk for making medical errors and other mistakes. Shortages in staff trickle down to patient care too. Hardly a day goes by when I do not hear someone say “I had to wait 30 minutes for someone to come and help me get back into bed.” When it comes to healthcare, people are not concerned with staff shortages when a loved one is hospitalized. Customer satisfaction is key to good medicine and community policing alike. And like police officers, a nurse or doctor who is on the last hours of a 12-hour shift is more likely to be ill-tempered and out of sorts. And like police officers, healthcare workers experience stress from long hours, shift work, and the nerver ending number of patients. Just ask any nurse or physician working in the emregency department and they will tell you it goes on and on round the clock. It is a mystery how some can stay in one job for any length of time given the current model of corporate medicine and the megagroup practice devouring one sole practitioner after another.
“The prolonged elevated cortisol levels that come with chronic stress and post-traumatic stress disorder (PTSD) can interfere with and damage the brain’s hippocampus” Wendy Suzuki author of Good Anxiety: Harnessing the Power of the Most Misunderstood Emotion.

The brain and body experience stress like a jolt of toxic hormones that have the power to gradually reduce the ability to relax and quiet the body. I am tasked with assessing employees following high acuity/high lethality calls for service who find themselves in an unsustainable state of physical tension and mental fatigue. I teach mindfullness and biofeedback strategies for people suffering with the effects of chronic exposure to high stress situations and the physical impact of these. When working with a group of medical providers stress may become overwhelming after a particularly stressful shift, like many hospitals experienced during the coronavirus pandemic.
I presented a conference on Stress and Healthcare providers: Caring for the Caregivers shortly after our emergence from the nationwide pandemic response in 2022. On that night, I wanted to bring some examples of current stress the frontline healthcare workers experience – especially with the pandemic now in the rear view mirror. In doing so I realized that even preparing for this 90 minute presentation was as much as I could handle with so much on my plate. I needed to remind myself, I am not a superman, I am not a warrior. I must take time for myself and cleanse my psyche of the evil spirits floating around in my unconscious mind. I am aware of the impact of stress on my thinking and my intimate life.
In the short term, our bodies need the adrenaline and cortisol to quickly activate our brains and other organs to react when a threat exists such as when a patient unexpectedly goes south. Since we were being chased my sabertooth tigers we have relied upon the “threat response” to keep us alive. In any environment our bodies need this fight-flight system to modulate and guide our behavior including when to run, fight, or freeze. It comes down to using our sensory system to be on guard for us and when we are exposed to something threatening, like a crash in our patient’s blood pressure or looking through a darkened building trying to find a burglar.
“If you exercise regularly, get good-quality sleep and take steps to reduce and/or manage your stress, “you can reduce stress activity in the brain, systemic inflammation and your risk of developing cardiovascular disease,” reported Ahmed Tawakol, a Massachusetts General Hospital physician quoted in Washington Post article on Stress published in 2022.
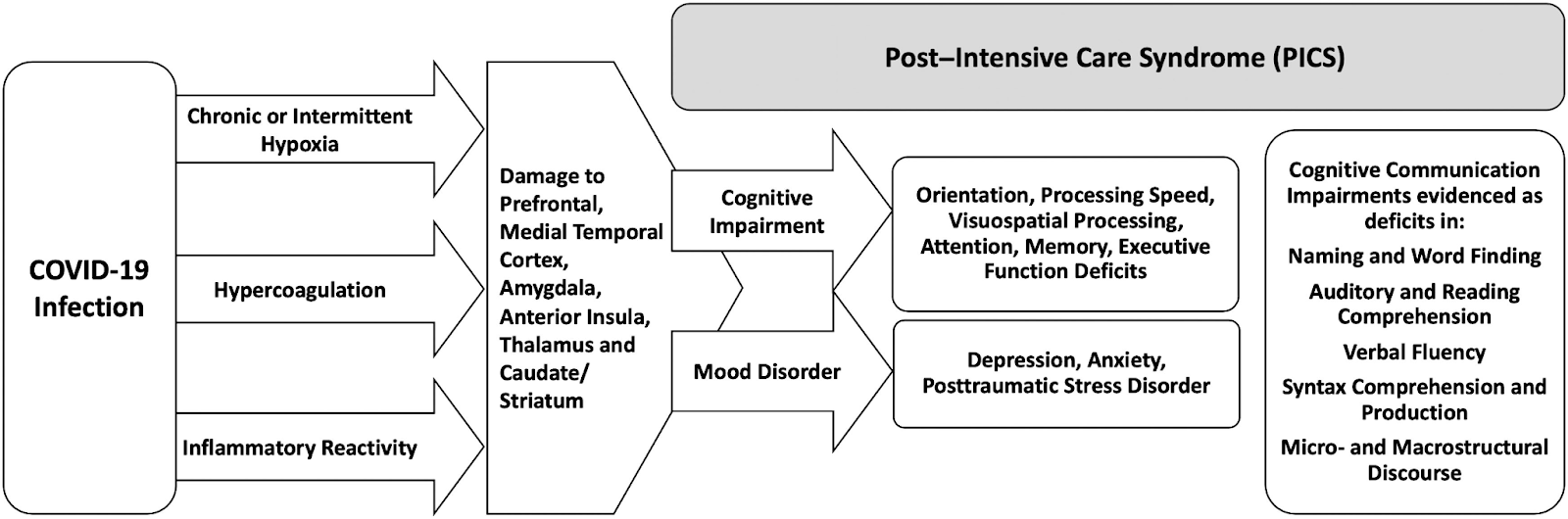
Chronic stress is hard on the human body. Most people who seek out a blog like this one are well aware of the toxic impact of an abnormal stress response. “The prolonged elevated cortisol levels that come with chronic stress and post-traumatic stress disorder (PTSD) can interfere with and damage the brain’s hippocampus, which is critical for long-term memory function,” Wendy Suzuki said in a Washinton Post article (2022). The hippocampus and amygdala are a constant filter for danger and threats to safety. Abnormal activation or damage to these organs leave a person struggling with constant activation of the fight-flight response that we know is unsustainable. Or even worse, we are left somewhat helpless without this cueing mechanism. When it starts to rain upon us and we do nothing to initiate staying dry or move away from the lightning. Long-term increases in cortisol can also damage the brain’s prefrontal cortex and its interconnective pathways. These are essential for focused attention and concentration, as well as the functioning of the higher order executive system needed for problem solving and other cognitive tasks we often take for granted. That is until they are corrupted by stress hormones running amock.
What are the signs of burnout? First, there are many nurses who have become numb and disinterested. Some career nurses pull the plug on their roles leaving to become a home health nurse or perhaps off to the nursing home nearest to their homes. Many experience caregiver fatigue and waning empathy from hours of high stress patient care and management. During the relentless pandemic Many want to go back to the “old way” of taking care of patients by using the primary nurse model which divides high acuity patient among the senior nurses on a shift. The primary nurse is usually repsonsible for attending team meetings designed to update physicians and consultants as to how treatment goals are being met.
Secondly, burnout can leave people exhausted, unmotivated, and cynical – the consequences of which can be catastrophic in many professions. As well as impacting professional growth, research suggests that these extreme stress levels can impair social skills, overwhelm cognitive ability, and eventually lead to changes in brain function and damaging physical disease and inflammation in vital organs leading to premature aging.
The stress of this is often overlooked. “During the pandemic began, newly minted residents who normally wouldn’t take care of patients with severe respiratory illnesses, such as those training to be psychiatrists, podiatrists, or orthopedic surgeons, have been asked to volunteer to work in COVID-19 wards” across the country according to a report by Deanna Pan in the Boston Globe on May 9, 2020. Professionals including residents in training, who ride a high stress career need time to process the trauma they face each day. That is not always possible. As a result, the cumulative impact can abbreviate even the most stalwart among us. Supportive supervision can assist young professionals to mitigate the impact of trauma and stress. Time for resilience should not be put off because of staffing shortages.
Working on the front lines with patients who are dying is horrific. This is especially painful when there is seemingly nothing that can be done to help them. First responders and frontline hospital workers are trained to provide emergency care. When their training is not effective, than feelings of helplessness will grow (Sefton, 2020). These feelings can be overwhelming. The cost has been great with increased rates of suicide since the shutdown began in March including those on the frontlines where the decisions they made both right and wrong may have been impacted by the unending stress of patient care.
On April 27, 2020 Lorna Breen, a physician specialist in emergency medicine took her own life after being witness to dozens of patient deaths during the peak of the coronavirus and contracting the virus herself and surviving it. Dr. Breen was a professional and emergency service medical director of NewYork-Presbyterian Allen Hospital and had no history of depression or mental health diagnoses.
More should be done for employees to assist them in remaining emotionally hardy and resilient for long-term career satisfaction. We know that days of stress from never ending patient flow can undermine career-oriented nurses and shorten their work life – something that no employer wants to see. The same as in law enforcement, finding replacements for nurses, doctors, and other caregivers is not easy. It is important to get ahead of career paths and lower the chances of losing the best and brightest because they are pushed too hard by a hallow system that does not care for its employees. Its human capital is the source of all business success. The loss of its human capital is the actual cost of stress and should be better addressed with thoughtful awareness, firm compassion, and kindness.




 The isolation felt by people in quarantine can leave the average person feeling numb and emotionally languished. Recently, I provided a zoom conference on the psychological impact of the coronavirus in November 2021 from my office at Whittier Rehabilitation Hospital in Westborough, MA. It was well attended, largely by people who are psychologically minded and aware of the points I endeavored to make. My target audience was the people who were struggling and vulnerable to decreased coping during covid-19 recovery. I am unsure we hit the mark I was hoping for with the target audience.
The fallout in mental health from the coronavirus is real and it is now recognized as a public health menace among recovering adults. It is now being seen in children and adolescents with growing concern. Just like younger patients, loneliness and social isolation in older Americans are serious public health concerns putting them at risk for dementia and other serious health conditions including failure to thrive, sepsis, malnutrition, addiction, and mental illness according to a CDC report. For many individuals in quarantine, the nightly happy hour started earlier and earlier raising the specter of worsening substance abuse and addiction. The liquor stores were soon to be considered essential services and package delivery became a common source of re-supply.
The impact of isolation, emotional loss, and social detachment undermines public and behavioral well-being across the life span. It is a co-occuring illness among illnesses afflicting millions. I see it in my own family as nerves are frayed now almost 2 years in – first noted in the blog post published in
The isolation felt by people in quarantine can leave the average person feeling numb and emotionally languished. Recently, I provided a zoom conference on the psychological impact of the coronavirus in November 2021 from my office at Whittier Rehabilitation Hospital in Westborough, MA. It was well attended, largely by people who are psychologically minded and aware of the points I endeavored to make. My target audience was the people who were struggling and vulnerable to decreased coping during covid-19 recovery. I am unsure we hit the mark I was hoping for with the target audience.
The fallout in mental health from the coronavirus is real and it is now recognized as a public health menace among recovering adults. It is now being seen in children and adolescents with growing concern. Just like younger patients, loneliness and social isolation in older Americans are serious public health concerns putting them at risk for dementia and other serious health conditions including failure to thrive, sepsis, malnutrition, addiction, and mental illness according to a CDC report. For many individuals in quarantine, the nightly happy hour started earlier and earlier raising the specter of worsening substance abuse and addiction. The liquor stores were soon to be considered essential services and package delivery became a common source of re-supply.
The impact of isolation, emotional loss, and social detachment undermines public and behavioral well-being across the life span. It is a co-occuring illness among illnesses afflicting millions. I see it in my own family as nerves are frayed now almost 2 years in – first noted in the blog post published in  I have worked with older clients for over 25 years first as a post doctoral fellow at Boston City Hospital – now BUMC. Long before the pandemic, my work at Whittier Rehabilitation Hospital has been to provide support and direct service to patients’ suffering from debility associated with decline in physical health along with the psychosocial needs and changes. All too often, this includes feelings of loss of control and sadness that is palpable in our short conversations. Many seniors feel invisible and the virus exacerbates these feelings. Declining health further instills the loss of purpose and amplifies the stigma of being seemingly infirm. The lack of purpose germinates from the passing of a spouse, close friends who move or have died, food and financial insecurity. It precedes a death wish and it’s associated demoralization. My mother was infected with the coronavirus in mid-April 2020 before the vaccine was introduced. She lived in the same nursing facility where I lost my 93-year old aunt in the first wave of the virus in May, 2020. My mother survived the virus but it has taken a significant toll on her physical and cognitive well-being. We were not permitted to see my mother during her illness and my aunt was alone on May 1 when she succumbed to the virus.
I have worked with older clients for over 25 years first as a post doctoral fellow at Boston City Hospital – now BUMC. Long before the pandemic, my work at Whittier Rehabilitation Hospital has been to provide support and direct service to patients’ suffering from debility associated with decline in physical health along with the psychosocial needs and changes. All too often, this includes feelings of loss of control and sadness that is palpable in our short conversations. Many seniors feel invisible and the virus exacerbates these feelings. Declining health further instills the loss of purpose and amplifies the stigma of being seemingly infirm. The lack of purpose germinates from the passing of a spouse, close friends who move or have died, food and financial insecurity. It precedes a death wish and it’s associated demoralization. My mother was infected with the coronavirus in mid-April 2020 before the vaccine was introduced. She lived in the same nursing facility where I lost my 93-year old aunt in the first wave of the virus in May, 2020. My mother survived the virus but it has taken a significant toll on her physical and cognitive well-being. We were not permitted to see my mother during her illness and my aunt was alone on May 1 when she succumbed to the virus.