Police agencies expend a great deal of LEO resources dealing with citizens with mental illness. The Washington Post (2015) and the Boston Globe (2017) both did large feature stories on police use of force against mentally ill persons. The profiles were gut wrenching but only one example illustrated the emotional toll on law enforcement officers who are involved in fatal use of force situations. This fact fails to illustrate the emotional toll officer involved shootings has on member of law enforcement. The Boston Globe Spotlight Series entitled The Desperate and the Dead was published in 2016. I have written about officer involved use of force for over 5 years now.
The interaction between poly-substance abuse or dependence and exacerbation of underlying mental health symptoms is complex. It must be studied. The interaction of the two is sometimes lethal as reported by the Globe Spotlight team. The focus of mental health advocates and criminal justice experts nationwide is to provide options for jail diversion. Programs like alternative restitution have reduced sentencing and have not reduced the police use of force. Lethal force results as a function of the behavior of the subject. His capacity to listen and follow directions guides the force that will be used against him when confronted by law enforcement. It is impossible to utilize de-escalation techniques in all cases of police-mental illness encounters.
I have featured some very troubling cases including a case of patricide in Vermont. In that case, Kryn Miner, 44 was shot and killed by his son in 2014 after threatening his wife and stating that he was going to kill his family. Ironically, Miner and his wife has just returned from a wedding. Kryn Miner was intoxicated and had both PTSD and a traumatic brain injury. He was on a waiting list for care at the local V.A. Miner threatened his family with a gun a year before his death but the event was never reported to police. Current and former police chiefs said that without large-scale police retraining, as well as a nationwide increase in mental health services, these deadly encounters will continue. The loss of veterans from suicide remains a significant moral shortcoming.
“When officers are faced with a deadly situation, when there is a gun pointed at a cop, there is no time to go into mental health measures,” SFPD Chief Grace Gatpandan said in 2015. Washington Post (2015) Lowery, W. et al. DISTRAUGHT PEOPLE, DEADLY RESULTS: Officers often lack the training to approach the mentally unstable, experts say
Gun violence is a public health problem. The American Medical Association is now recommending physicians ask their patients whether there is a firearm in the home. Especially among older adults, divorce and substance abuse contribute to the risk of suicide by means of a firearm. This information may raise physician awareness and set off warning signs especially in patients without social support. According to David Rosmarin, M.D. at McLean Hospital in Belmont, MA – Rampage violence or spree violence is rare but always sensational- “violence is the currency of what we do” so MD’s need to become comfortable with the conversation about violent intention. The serious mentally ill account for only 3-5 % of all US violence – substance abuse is a big factor in violence according to Rosmarin. Violent intention is frequently communicated in advance. “There were signs along the way that were ignored” according to Rosmarin. These signs may be important when building systems of care and training LEO’s who are expected to de-escalate dangerous citizens and with limited training.
“I called 911 so they could disarm him, not kill him,” Joan Hart told a reporter in 2007 after her suicidal husband, James, 65, was fatally shot by Quincy police in their backyard after charging officers with a knife. Boston Globe Spotlight Team 2016
The quote about is heart breaking because the outcome of that call for help was not good. All officer involved shootings are carefully investigated as part of normal protocol. People fail to appreciate the impact the OIS has on the officers involved. No police officer leaves his house with the intention to get into a gun fight. “There will always times when police officers encounter those with mental health needs especially in times of crisis and social disorder. Training and education offer the best hope for safe and efficient handling of cases. A continuum of options for detox, dangerousness assessment and symptom management must be readily available – but sadly here in Massachusetts they are not” Sefton, 2016
___________________________________________ Boston Globe Spotlight Series (2016) Desperate and the Dead. Washington Post (2015) Lowery, W. et al. DISTRAUGHT PEOPLE, DEADLY Sefton, M. (2016) Human Behavior blog post: https://msefton.wordpress.com/2016/03/24/deadly-force-continuum-changing-officer-safety/ Taken June 4, 2019
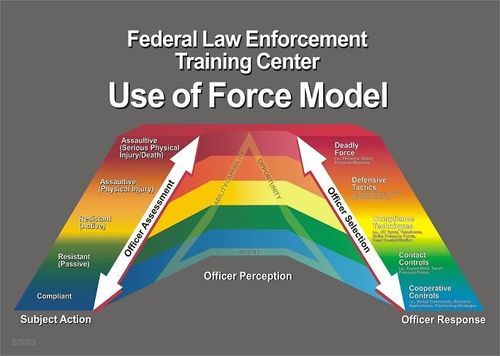
 The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.
The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.