WESTBOROUGH, MA January 2, 2017 I grow contemplative with the change of each calendar year and wonder where the time has gone since 2000 when one of our closest friends dressed as the pink millennial elephant and danced on the front yard to the delight of the four boys who were stuck at home with nothing to do. It was a big surprise to us all and was meant to make us laugh and bring joy. I cherish these friends and am fortunate to have so many more. For those of you who regularly read these posts I wish you all a happy new year – one that is safe and prosperous. I expect that most people wish others peace and prosperity on New Years Day.
Intuition and deviance
I know there is a subset of people who may not be who they would have us believe they are. The world has seen unconscionable acts of barbarism in lone wolf terrorists in 2016 that I will not revisit here. Deviance comes in many forms of disguise. Workplace violence is nothing new and continues to be on the radar screen of human resource and security experts. Vester Lee Flanagan, 41, a disgruntled television reporter killed WDBJ colleague Alison Parker and her cameraman as she did her job on live television. He had been escorted off the station property following repeated attempts at bullying the people he worked with in Roanoke, VA in summer 2015. The live twitter posts, videotaping the shooting, and horrific execution of the victims by Flanagan will be a specter for years to come. People may have anticipated this behavior by looking closely at his prior employment patterns and behavior that were highly erratic. Mental health advocates might argue that Flanagan had depression or some other debilitating psychiatric illness that he chose to ignore. In his 23 page manifesto he cited discrimination, harassment and bullying as the reason for his actions.
“Like dozens of mass killers before him, the shooter embodied a deadly mix of resentment, delusion, and thwarted aspiration” according to Sarah Kaplan (Washington Post, August 27, 2015).
Each of us needs to be aware of our environment and the possibility of a wolf in sheep’s clothing in our midst. Do not be surprised by the behavior of wolves – especially those looking to feed their hubristic conceit. Relationship and intimate partner violence takes on special significance in this new year and there are well documented red flags that forewarn offering a glimpse of the wolf lurking below the surface flash and excitement of what is new. Gavin deBecker offers the textbook – The Gift of Fear as an essential reminder for each of us to closely be aware of our inner feeling states such as the sense of fear – when in the presence of those who might do us harm. Understand fear as a prehistoric memory trace genetically programmed into each of us. It allows us to feel a warning as the wolf gets us in his sites. deBecker owns a security firm that provides employee threat assessments and interviews victims to see what they were thinking and feeling before being attacked. Many reported an odd sense of foreboding just before being assaulted or attacked. By listening to and acting on one’s internal sense of fear you may save your own life.
The possibility of home-grown violence erupting in the life of the average American is greater than ever before. As recent events have illustrated there are marginalized people living on all sides of us – some of whom are brooding – blaming. The reasons for homegrown violence: relationship and workplace violence are very complex and beyond the scope of what can be explained in these pages. As a society the identification and containment of those who depravedly evoke fear in others is requisite to social order. The next generation of leaders should find a balance between public safety, treatment and rehabilitation for those living with mental illness and ardent protection from the brooding haters who dress as sheep in order to make us afraid and bite our throats.
Happy New Year and be aware of your surroundings and watch for the wolf in sheep’s clothing.
WESTBOROUGH, MA December 29, 2016 I have long been an advocate for prompt and comprehensive treatment for those afflicted with mental illness. Now police are increasingly linking up with mental health agencies as a way of diverting mentally ill person’s from jails into treatment for their emotional affliction. In my experience this is no easy task. In some cases criminality and mental illness are not mutually exclusive. Some who suffer with emotional issues like bipolar depression, drug addiction or anxiety may respond poorly to treatment and may need containment. Those most refractory to treatment often become most difficulty to manage in society. The untreated mentally ill have a higher rate of violence than those in voluntary treatment.
As early as 1984, I served the pediatric population in Boston at the Boston City Hospital Pediatric Emergency Department as the on-call clinician in psychology. That same year I was appointed to the ED at Hale Hospital in Haverhill, MA for screening people in crisis. Those who were stable and had support systems in place would be released – usually with an outpatient referral. Meanwhile, patients without at-home safe guards who could not plausibly answer the question “what brought you to the decision to harm yourself?” were admitted to the hospital. Other mitigating factors like healthy living arrangements, employment, sobriety, and no history of suicidal behavior were positive indicators of future outcome. It was a position I loved and is an important clinical role to this day across the United States. Later as a community mental health psychologist in Long Beach, CA, I served the Children’s Service as someone charged with screening adolescents in crisis living across Los Angeles County. In each of these locations I worked closely with social workers, case managers, police and gatekeepers at state and county psychiatric units to find open beds for kids in need.
In 25 years since there has been very little innovation and fewer still treatment beds for those in need. Today’s depressed and emotionally wounded often spend days in emergency department hallways further wounded by a demoralizing system of delivery that is overwrought and has no place to send them. This scenario was the case in 1985 and remains the case in 2016. In Massachusetts and counties across the United States publicly funded hospital beds – including state hospital beds have been eliminated. In the 1970’s and 1980’s the pendulum of advocacy swung toward community-based care and away from hospital-based treatment. This left the chronically mentally ill without a support net for treatment, medication management and long range hope. Many became homeless, unemployable and abusive of drugs and alcohol.
Police provide frontline intervention – often with little training
Police officers became the first line of defense as the hospital beds were eliminated. The mentally ill and those addicted to any number of drugs or alcohol grew homeless and sometimes menacing as they struggle with symptoms. Now police officers are being trained to intervene with these marginalized citizens with crisis management skills. This poses a conundrum for the current zeitgeist of community policing theory in that the notion of dangerousness relies on critical scrutiny of the underpinnings of human behavior and often nonverbal indices of psychopathology. Some believe this is state of the art police science. Departments from Augusta, Maine to Los Angeles, CA to San Antonio, TX are using frontline officers as crisis resolution specialists for police encounters with the acutely mentally ill. Many are paired with licensed clinicians while others are working the streets alone.
The collaboration between police and mental health personnel is not new. But the use of police officers as crisis intervention specialists is innovative and gaining traction in many places around the country. Yet these officers must always be aware of the uncertainty of some encounters with police and those suffering with paranoia or psychotic, illogical delusions, PTSD, or traumatic brain injury that may not respond to verbal persuasion alone. Decisions about when to utilize greater force for containment of a violent person is sometimes instantaneous.
The use of force must be fluid and officers in the field are expected to modulate the force they apply to the demands of the situation and be ready to respond to changing threat levels. Michael Sefton, 2015
In 2002, I was appointed to a Massachusetts police department having once served in southern Maine right out of college. As a psychologist I made an effort to bring mental health concepts into police work without much fanfare or interest. Mental health topics are not as sexy as defensive tactics or firearm training, I was once told, so finding numbers was sometimes tenuous. There are still many myths about intervening with those who are making suicidal and homicidal threats and training opportunities are taking on more importance. Especially these days. Suicide by cop became a phenomenon that no officer ever wants to confront. All violent police encounters guide officer behavior. “The degree of response intensity follows an expected path that is based on the actions of the perpetrator not the actions of the police” (Sefton, 2015).
Suicide by cop – predicting behavior
In the 2014 FBI Bulletin, Suicide by cop (SBC) is defined as “a situation where individuals deliberately place themselves or others at grave risk in a manner that compels the use of deadly force by police officers” according to Salvatore, 2014. This happens more than one might expect and is often preceded by rehearsal events according to Salvatore. “Suicide rehearsals are practice for the attempts that will follow within a few hours or days. SBCs may be tested. Officers should use caution when recontacted by an individual who previously presented signs of mental illness, had no need for assistance, was standoffish when asked what was needed, or was anxious to assure the officers that everything was fine. The initial contact may have been practice for an SBC.”
The best predictor of behavior is past behavior. The prior demeanor that police have observed in those frequent flyers who pop up on police radar over and again often sets the stage for violent conflict later on. But not always. Situations grow exponentially more grave in the presence of drugs and alcohol raising the level of lethal unpredictability. For many struggling with depression or other serious mental illness being sober or drug free can be the healthiest thing they can do for themselves. The uncertainty of the SBC scenario makes the likelihood of a successful de-escalation a tenuous exercise in the life and death force continuum.
The motives for SBC are multifactorial and undeniably linked to poor impulse control associated with drug and alcohol intoxication. The triggers are identified by Salvatore as “individuals who feel trapped, ashamed, hopeless, desperate, revengeful, or enraged and those who are seeking notoriety, assuring lethality, saving face, sending a message, or evading moral responsibility often attempt SBC”(2014). Some believe they will become famous and earn large monetary settlements for their surviving families following a SBC scenario. Other victims are tortured souls who make no demands and offer no insight into their suicidal motive and are killed when they advance on police or turn a weapon toward responding officers.
Training in police-mental health encounters has slowly taken hold. This innovation in community policing offers hope for reducing fatal encounters. No amount of training in crisis management will reduce incidence of SBC to zero but ongoing training to identify the behavioral indices of imminent violence, psychosis, and suicidal/homicidal ideation will reduce these lethal encounters. Most officers are highly skilled at using their verbal skills to de-escalate a violent perpetrator without using lethal force – even when a higher level of force may have been warranted.
WESTBOROUGH, MA January 7, 2017 What happens once the “scene is safe”? Usually the hostile threat is taken into custody – either to jail or a hospital. In the aftermath of high stress events such as talking a violent alcoholic into surrendering there should be an opportunity to follow-up and bring closure. In the time it takes to defuse a potentially lethal citizen encounter the police officer has established a connection – however slim it may be. Aftermath intervention may go a long way to further validate the first steps taken with the initial encounter. With such high incidence of polydrug abuse the threatened violence may take on a surprisingly banal theme and the importance of sobriety may be realized once the scene is safe.
Most officers are already highly skilled at using their verbal skills to de-escalate a violent perpetrator without using lethal force – even when a higher level of force may have been warranted.
I have been called to the same home over and over when a violent adult male became intoxicated and gradually overwhelmed and depressed. Each time officers went to the residence there ended up being a fight. We deployed OC spray on more than one occasion each of us getting the pepper in our eyes. This man was hooked up and sent to the hospital time after time. Upon his return (usually within 1-2 days) he would have a short period of sobriety and slowly start drinking and abusing his father again resulting in the same battle we had days, weeks, months ago. Interseting to me was that the younger man was quite reasonable when he was sober. He had no interest in seeing a therapist – nor could he afford one. The important question to me was what steps could be taken to link this guy to a 12-step alcohol (and drug) recovery program? There were meetings in our town and they were free. I thought if he could meet a sponsor than hs abuse of his father might be reduced. In any case, sooner or later someone was going to get seriously injured on a call at this home. We had heard rumors of him wanting to commit suicide by cop.
Community policing has long espoused the partnership between police and citizens said Sefton in December 2013. The positive benefits to this create bridges between the two that may benefit officers at times of need – including the de facto extra set of eyes when serious crimes are reported. The same goes for crisis management. The relationships you build while in the community can serve to help soften the scene and slow down an escalating person of interest who may be looking for a fight. Violence often occurs after a period of brooding isolation that is fueled by alcohol and a bolus of rage.
Police officers are regarded as the front line first responders to family conflict and DV. Now they are being trained to better interact with those thought to be mentally ill. For better or worse, the police have an opportunity to effect change whenever they enter into the potentially hostile foray. This affords them a window into the chaos and the opportunity to bring calm to crisis.
“… He stood in the doorway with a loaded gun and talked about killing himself and/or children and myself. He was bringing up old verbal threats and I thought they were going to come true”
Amy Lake – from July 2010 order of protection
The words above were taken from a requested order of protection in the state of Maine in 2010. The threats upon this victim and her family became a reality exactly one year to the day after this order was put in place in 2011. Amy
Michael Sefton
Lake and her two children were murdered by her husband Steven Lake who killed himself as well. Immediately following the killings a Maine district attorney said “there was nothing we could have done to prevent these killings”. These were the words that triggered a team of professionals including myself to research the sequence of events that lead to this event. A formal psychological autopsy was undertaken in 2011 following these murders and over 50 recommendations were generated (Allanach, et al 2011).
I am sick to my stomach as I write about another senseless killing of Wanda Rosa in Methuen, Massachusetts in late summer 2016. The case resembles so many cases of domestic violence homicide – manipulation and control. Ms. Rosa had a permanent order of protection but had recently modified the order to allow Emilio Delarosa to see the child they had in common. Why in the world would anyone allow Delarosa to see his son? He is no role model and the potential for terminal violence was readily apparent as depicted in the order of protection. He expressed his intent to kill his girlfriend on more that one occasion. Delarosa’s history of intimate partner violence had risen to the level of a permanent ban – signaling that the pattern of violence was undeniable and the red flag indicators for domestic violence homicide (DVH) were apparent in the eyes of the police and judiciary when the permanent order was granted.
Permanent orders of protection are rarely granted unless the pattern of violence was so prevalent and unremitting that the potential of harm or death to the victim and her family was unsurpassed as in this case. It is known that Delarosa was manipulative and controlling of his girlfriend getting her to drop charges over and over and later alter the terms of the restraining order – ultimately resulting in her death. Secondly, the person against whom the stay away order is granted must have demonstrated a blatant indifference of the order of the court by having recklessly violated the order over and again. It should not have been altered. In the past 18 months cases meeting these requirements (such as this one) have resulted in intimate partner violent deaths. The Jarod Remy 2013 murder of Jennifer Martin is a despicable reminder of the need for change in cases of DV. Remy killed his girlfriend by stabbing her multiple times as the couple’s 4-year old child bear witness. In spite of laws designed to reduce the likelihood of DVH Rosa was not adequately protected.
Rosa’s boyfriend Emilio Delarosa is on the run as of September 20. He is accused of murdering his former girlfriend after years of abuse, strangled her to death as their 4-year-old boy pleaded with him to spare her life, according to court records. “No Dad” the child was heard to say over and over. As in the Remy case, the 4-year old witnessed his father choking Wanda Rosa until she was dead.
“I suspect there is a strong likelihood that he too will be among the deceased in the coming days as is the common eventuality among those who commit the unconscionable, violence that manifest in this terminal event” according to Michael Sefton, Ph.D., director of psychology and neuropsychology at Whittier Rehabilitation Hospital in Westborough, MA. When some men violate the permanent protection order it is the result of unbridled rage and defiance against a “system” they believe has failed or unfairly humiliated them said Sefton in a release. They are murderous and often turn their rage inward in an act of suicide. I would look for the triggers of what set Delarosa’s terminal rage into action. It could be something as simple as being told he needed to have monitored visitation with is son or learning that the female was seeing another man – both conjectural on my part. After the alleged killing Delarosa was heard to say “It’s over, it’s over, it’s over” when speaking to his sister.
“This is the complexity of domestic violence and the cycle of abuse,” said Arelis Huertas, who oversees domestic violence and sexual assault programs at the YWCA of Greater Lawrence. “Many survivors say, ‘He’s a great father, he was only abusive toward me.’
“Domestic violence is not random and unpredictable. There are red flags that trigger an emotional undulation that bears energy like the movement of tectonic plates beneath the sea.” according to Sefton. A psychological autopsy should be undertaken to effectively understand the homicide and in doing so contribute to the literature on domestic violence and DVH according to Michael Sefton who with colleagues published the Psychological Autopsy of a case from Dexter, Maine where a father murdered his child, estranged wife and ultimately himself (Allanach, et al, 2011). In the days preceding the murder there are usually red flags or pre-incident indictors that people see that signal the intentions of the murderer. These clues provide police and the judiciary with data to craft protection plans and are the commonalities found in cases of DVH across the state and across the world. Some red flag behaviors signal the emergence of imminent terminal anger that can be seen in the social media accounts of intimate partners who go on to kill their spouses. I am quite interested in the compelling reasons that Delarosa may have argued that resulted in the change in the permanent order of protection. The outstanding Boston Globe article about the slaying is a sad reminder of the early warning signs of DVH. All the red flags were present. In a blog published in 2013 I list the tell tale warning signs of intimate partner homicide and the need for tougher bail conditions (Sefton, 2013).
The impact on the child will be lifelong. At age 4, children are developing their sense of gender identity in the setting of developmental growth, cognitive maturity, social functioning and continued individuation. Imagine the child who is reunited with his parent after a period of mandated protection due to DV. He is now able to see his family and may be fraught with both excitation and fear. It would be normal for the child to have fantasies of reunification of the family and perhaps self-blame for not having stopped the action of his father. Just like the daughter of Jennifer Martin and Jarod Remy this 4-year old boy will forever be reminded of the life he will not have.
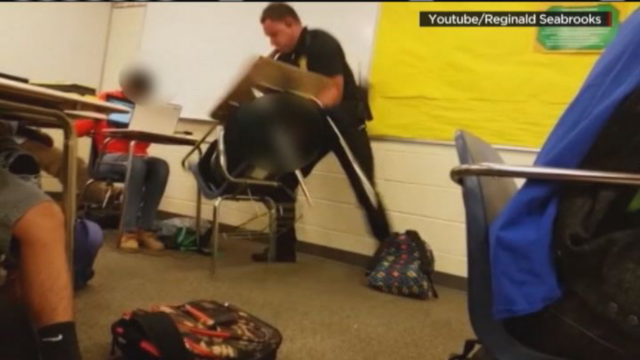
WESTBOROUGH, MA October 28, 2015 “To say that it is because they lack training in techniques of crisis de-escalation that some deaths may have been prevented is unfair and short sighted.” This quote was first published in the summer 2015 when people (perhaps in the media) first started calling for police officer training in mental health awareness and de-escalation training for police officers. One source actually suggested providing more training in mental health de-escalation and less training in the use of force – including firearms. Some wrongly believe that this “sensitivity training” will reduce the number of officer involved shootings with those who are known to be mentally ill. Unfortunately police shootings of mentally ill suspects has been on the rise in the past 12-18 months. Yet the use of force in police work continues to enter the collective consciousness when images of police officers acting aggressively toward defiant high school student go viral on social media.
School Resource Officer take down of resistant student from posted You Tube video
Arguably, when the police are called to keep the peace or investigate a violent person call they are required to meet this threat with heightened vigilance for personal and citizen safety. When a violent person is encountered the use of force continuum comes into play. In the case of the Columbia, SC high school student who was aggressively choked and slammed to the floor while seated at her desk, the school resource officer was rightfully fired. The student posed no immediate threat such that hands on tactics were required to control a menacing suspect. In this case, the student was angry at being told she needed to put away her cell phone and was defiant to teacher direction. The police were called to the classroom as a show of force when neither the teacher nor the administrator could redirect her behavior.
If the violent person is actively aggressive or menacing with threat of lethal injury to the police or others than there is unlikely going to be any successful de-escalation until the threat of lethal force is eliminated. If the violent person responds to officer directives to cease and desist all violent action and submit to being taken into protective custody or arrest – only then can mental health assessment be initiated. At the moment of crisis the need for public safety in all violent situations supersedes the individual need for care of a mentally ill person. In the case of the South Carolina high school student no such threat existed but non-physical tactics were ineffectively deployed. The officer may have been able to diffuse the situation with empathy, understanding, and firm authority. The arrest could not be made without a higher degree of force for an actively resistant student that first punched the police officer.
Sefton, M. (2015) Blog post taken 10-28-2015 https://msefton.wordpress.com/2015/08/23/calling-for-de-escalation-training/
WESTBOROUGH, MA January 20, 2015 Dementia is a life changing affliction for both the patient suffering with the neurocognitive decline and spouse and family members alike. Caregivers have a particular cross to bear – especially those without support. It is a highly stressful role for any spouse that requires both education and support. They are at high risk for burnout otherwise known as caregiver fatigue. For anyone who has had a loved one suffer with this disease “it is like seeing a family member die slowly, daily, withering away into an empty vessel” according to Michael Sefton, Ph.D., Director of Neuropsychology at Whittier Rehabilitation Hospital in Westborough, MA. “It is very important to obtain a careful and sound neuropsychological assessment of patients’ suspected of having dementia because so many conditions mimic dementia and may be treatable” according to Sefton.
When a caregiver is overwhelmed something must be done to provide emotional respite for the spouse or family member. Caregiving spouses frequently have powerful feelings of guilt, anger, and sadness as a result of seeing a loved one become forgetful, detached, and confused. They can be extremely difficult to managed in the home setting and sometimes require specialized day treatment. The decision to hospitalize or seek nursing home admission for a family member is an individual one. It is critical to look at the functional change in the afflicted family member and see what placement options make the most sense. Caregiver fatigue places afflicted patients at greater risk for neglect, battery and abuse than other medically complex cases. It places caregivers at risk for health problems of their own.
Throughout America, physicians and psychologist alike are mandated reporters for cases of suspected abuse – regardless of whether the caregiver is experiencing caregiver fatigue or not. Family members are strongly encouraged to support parents, e.g. respite care for afflicted parent, whenever one is suffering from a severe illness like dementia. Read the post at link below.
Lena told me she grew up in East Germany – behind the iron curtain from which she escaped when she was 33. Her best memories were from a time when Hindenburg was the country’s president. She lived in East Prussia near the Polish-Lithuanian border where most East Germans were Lutheran. As children, they were made to stand under the “Hitler cross” each day before school and recite the Socialist pledge for nationalism that she cannot forget. She recites the narrative for me in her native German – translating the final few words into English – “the flag is more important than the dead” she mocked shaking her head. Lena had an unexpected and compelling history about which her doctors seemed unaware.
They were driven from their homes by the advancing Red Army during WW II in the 1940’s as millions were. Yet, these East Germans were subjected to despicable atrocities most people are not aware of during the evacuation. “They took our homes. The banks were all closed. We had nothing” becoming tearful. I bear witness to Lena’s personal memories – the narrative of her life living under the Hitler cross and the journey to America.
Now 91, she lives alone since her husband died over a decade ago. She lives 70 miles from her daughter. I was asked to interview Lena and determine if she was capable of returning to her home alone after she sustained a fall and broke her humerus – the long bone in her arm. It was the second time she had fallen in the past year. I reviewed the chart and her nurse commented that she is noncompliant and suspicious somewhat randomly. It was my role to provide an understanding of Lena’s cognitive status for the treatment team with some pithy explanation as to why she keeps falling and whether she can go home again.
Lena is frail in appearance and has a small frame. Her eyes are hard and I cannot tell what color they are. Her white hair is wispy, thinning. She is sporting a blue sling that keeps her shoulder from moving. It is her dominant arm I note with some reluctance. Sadly, I wonder if the traumatic recitation I am now hearing may be a sign of the psychic unraveling that some elderly trauma survivors experience shortly before death.
As a consultant I try to remain dispassionate. I need to determine her orientation, awareness of illness, capacity to concentrate, and review her gait training, balance, and daily carry over. I find Lena hard to redirect but I need to respect the urgency of her thoughts while she painfully unburdened herself. I am not optimistic about her returning home.
Moments of pleasure
Lena wants to go home so she can maintain her small garden in which she plants tomatoes and colorful flowers each year. “People admire my yard and sometimes stop to take pictures of the flowers” she reports with a slight and hopeful smile. She even boasted a one-handed technique used to plant her garden last year after suffering a shoulder injury in her first fall. With her left arm she dredged an orifice just large enough for the seedling. Then with the heel of her foot she covered and packed the plant with great acumen and apparently admirable results. Resourceful and independent, I thought bringing new meaning to the green thumb adage.
Unfortunately for Lena, there is more than just making her garden she worries about. She is afraid about what might happen to her home when she isn’t there. There has been vandalism – “they painted the Hitler cross on my mailbox and house and broke my windows” she reported indignantly. “What can you do” her voice trailing off. Once, she paid some boys to shovel the driveway. They convinced her to pay them before the job was done and ran off taking her twenty dollars leaving only the snow behind. The same thing happened with the landscapers who she had hired to rake the leaves this fall. Can she go home again? I could derive little experience of joy in her history – often an outward sign of depression.
Lena was raised on a farm, I learned. But she had a brief childhood marred by atrocity and abject savagery. She was one of 9 children. “We had horses and cows and an orchard” she reminisced. Lena was brought up Lutheran but had Jewish ancestry. “Her mother was very religious” she described. Because they had property, landowners were expected to attend regular community meetings during which her father often spoke out against the government – against Hitler. “They had an eye on him when he came home from the war” she reflected. “They came and beat him up once, she remembered – somebody told on him” referring to the time he spoke out against the war at the community meeting. His battered and bruised body “looked like a rainbow” when describing his wounds. “Hitler did not grow up a German – he moved from Austria and promised to spread the ‘German way of life around the world'” she mused. “All he did was invent the autobahn”, now her bitterness and mistrust began to show.
Traumatic Losses
Lena saw 15 members of her immediate family murdered. Her father was shot to death in the orchard behind the family home when she was 9 years old by the German secret police because he spoke out against Hitler at a local meeting of property owners. Her 7-year old brother was made to watch. Her 4 older brothers were conscripts and died in the war. Lena said that her grandmother married a Jew. He was very nice, she pleaded. Later, the family home was taken from them and the animals were killed during the evacuation of East Prussia late in the war. By then she had already lost her parents. Neither the Germans nor the Russians were humane to the native population of Lutherans and Catholics, and Jews.
After being forced from their farm, Lena was committed to a warehouse to live. It was one big room. She was made to sleep between similarly damaged souls – many who succumbed – leaving their postmortem remains for others to see. She and her sisters were raped. Elderly women were raped and murdered. “People don’t know” she grieved now bearing witness to spectacles no person should ever see. She described the dreams she has to this day – of being trapped in a room with no escape but would go no further.
I return the next day to see what carryover she has of our first emotional conversation. I notice Lena sitting next to others in the community room – intrepid – yielding no outward sign of her inner torment. She spoke to no one with a glower on her face that could dissuade even the most confident salesman. She nodded and smiled slightly – faint recognition, I predicted. Uncertain. We agreed to meet again later in the day after bingo. I had been strongly impacted by her disclosure and felt I needed to hear more. What had happened to Lena since coming to America? Was she a member of her community? What kind of life had she built here in New England?
The promise of a better life brought Lena and her husband to America in 1952. She had one daughter. Her Lutheran beliefs taught her the importance of helping others in her community – even neighbors on Cape Cod, MA where she still lives. But the efforts made by she and her husband were often not returned in kind. People were not friendly and welcoming so soon after the war.
“My husband was a teacher in a technical school (in East Germany) and used to help the man who lived behind us when his car would not start” boasted the frail woman with a strong German accent. Here she expressed her bitterness at being persecuted by those who were ignorant and prejudice against people who are different – perhaps more so toward immigrants from Germany when they first arrived after WW II. “Kids don’t know about it today” she complained. She worried that the abject trauma she experienced during the second World War would one day become irrelevant – forgotten.
Secondary Trauma
The pain she felt in Germany was not eased by the democratic change of scenery. In fact, Lena herself was accused of killing Jews by a neighbor simply because of her country of origin. Her daughter was bullied and abused between school and home. The child’s principal refused to allow her to come and speak to the students to help them understand that she too had Jewish blood and had suffered unspeakably at the hands of the Nazi’s and those who drove them out. She wanted to protect her only daughter from the hatred and vitriol and suffering she had endured.
“I am responsible for what happens here in school,” said the child’s principal, “not for what happens when she leaves the school grounds” in a despicable collusion of denial and lack of courage. More than anything Lena wanted to shelter her only child from the same truculence she endured and make a better life than the one she knew. She didn’t even know Hitler” she cried, now rocking slightly.
Lena described a time when her husband was burned by acid that had been mixed into the water he used to wash his hands while working a stint in a local automotive garage. Afterward, he was sent to a physician who indicated the condition of his hands was a disease brought with him from their country in an outrageous distortion of the truth.
“You can complain to nobody” she bristled. “The police don’t do anything” she bemoaned. After her home was vandalized, one officer asked “What do you expect us to do sit in the driveway?”
Can Lena go home again? I am sure Lena would love to return to the idyllic family farm with the orchard and horses the way she remembers it before the Hitler cross flew above her school yard. To visit with her large family before the time when her father was murdered and her windows were broken and her mailbox was disgraced with the Hitler cross. Who can you tell, nobody knows what happened anymore?
I cannot envisage a life-like the one Lena has had with its childhood trauma, loss, and recurring prejudice and persecution. Yes, I would expect that Lena is suspicious and mistrustful but she is not paranoid. What would anyone do if they experienced the life events and atrocities experienced by this woman? The emotional resilience Lena has shown raising her daughter and making a home for her family has inspired me to look at her differently than others might have done in my position.
Lena should go home and yet she is at risk of falls when alone. She has fallen and broken both the left and right shoulders – unsteady on her feet. Her fear and anxiety stem from an underlying sense of vulnerability based entirely on her history of personal trauma and abuse while living under the Hitler cross. The reason for her noncompliance and emotional detachment are the predictable product of her early beginning in East Prussia near the border with Poland. It represents her fiercely stout-hearted spirit and enduring strength – features of the emotional veneer that are the underpinning of her being. It would be wrong to remove her from her place of safety and take her from the garden she loves that brings her a few moments of joy each summer. She feels pride in the tomatoes and colorful flowers she has grown for others to stop and see and sometimes even take pictures.
I return yet again to visit Lena and clarify some of her story and see how she is progressing. In what city did she live?How had she coped with the trauma of her life? When I enter her room I notice an aide rounding up the sheets and blankets from her bed. “She has been transferred to a nursing home,” he remarked without emotion. She had been discharged only a few minutes before I arrived. Her doctor believed it was the safest thing to do. Her daughter agreed I suppose.
For whatever reason Lena felt safe enough in my presence to share the narrative of her life over the course of a couple of weeks. I made an effort to deconstruct the mistrust she projected and summarily to lessen her emotional burden. Arguably, I was unable to extract a pithy aphorism that would send her homeward based on my impression. Yet I wanted to explain the rationale for her transfer. I am sure she was dispirited about not going back to the Cape. Again conscripted into battle over personal control and humility forced to sleep once more among the damaged souls. “Nobody knows what happened” Lena might say – but I do now.
“Whether or not a student receives support on an education plan has no bearing on the kind of support they might need when they return to school after a concussion” Michael Sefton, Ph.D. Director of Neuropsychology – Whittier Rehabilitation Hospital
Students who return to school following a cerbral concussion often require specialized scheduling, rest breaks, reduced work load, and other individualized support.
The debate over life and death often focuses on the heart and the brain. Some believe life ends when the brain ceases all activity – a term called brain death. Others believe death results when the heart ceases to beat. In a blog published in January 2014, the mind-body dialogue was discussed by Michael Sefton. He described the rudimentary force of life as the heart’s beating “which begins and ends with the inimitable squeeze of the cardiac muscle.” For patients who are being monitored the experience is highly stressful and often evokes fear and dread.
The link between what happens to our body and its effect on our mood and feeling state is well documented. Just as we must adjust to the early developmental changes of our children so must we adapt our own thinking and lifestyle to the changes brought about by the empty nest. Events such as having children leave home and head off to college and other events associated with empty nesting require flexibility and adaptation of roles for success. These important transitions signal an advancing age that sometimes accompanies physical decline in health and body. With that said it is important to note that many American’s are living healthier lifestyles and thus preserving physical health well into the eighth and ninth decades of life.
“Don’t ever get old”
Retirement was once described as a period of “golden years” and was thought to represent the final stage of one’s life during which the experience of freedom and contentment proffered a whimsical enjoyment of lazy, carefree days. It meant taking time to share one’s wisdom with those who are younger and pass on the stories of family, culture, and life itself. This is often not the case and I have had patients suggest that I should never get old. Retirement is frequently a time of unbearabe loss and despair.
One factor affecting quality of life is the sense of physical well-being. Retirement sometimes triggers an erosion of physical health and cognitive stamina choking all remaining time with recurring, monotonous doctor’s visits and tests. In truth, what may be a glorious time is now marred by fear and trepidation about one’s health, financial stability and declining physical longevity.
Poor cardiovascular health is an underlying cause of many chronic disease processes like stroke, diabetes, and auto immune disease. Heart attack remains among the leading precursors to early death and researchers are racing to uncover treatment options including early identification of those most at risk and life saving surgery to open clogged arteries. Meanwhile, people should take greater responsibility for their own health by eating better and building exercise into their changing lifestyle. Things like moderating use of alcohol, 7-9 hours of nightly sleep, and eating plenty of fruits and vegetables become the specter of truth and failure to an ever-growing problem with obesity. This is an important lesson for young adults to discover but is easier said than done.
The mind-body dialogue is one that matches wits with any great debate. What are the best methods for identifying ‘problem’ hearts before they reach a penultimate, fibrillating finale? Some doctors ask their patients to wear special monitoring devices – little boxes attached to the skin that permit the ongoing monitoring of life threatening changes in rhythm. Patients sometimes wear the monitor for a month or more. These monitors have the potential to catch irregular heart beats and allow physician’s to see a patient’s electrocardiogram on a minute to minute basis. The monitor requires that the person wearing the device to upload his data via a telephone line each day sometimes with little to no training. Each recording represents a cardiac event that the person wearing it is asked to chronicle in terms of action and feeling state when the device is active. The events are uploaded via telephone land lines in real-time that seems almost tortuous to those bearing the burden of wearing the device. The rhythms are quickly edited, analyzed and more often than not result in nothing more than a friendly vote of confidence – “you’re all set”.
Event Monitoring
Greater thought and training should be afforded to patient’s wearing event monitors. As time goes on most patients become accostomed to the vagaries of the heart and the sound it makes – lub dub, lub dub. The event recordings come in one after another and become part of the month-long survey of heart activity. Some people call two and three times daily worried that they are having a serious cardiac event. After 30 days the monitor is turned in for analysis by the cardiologist. These daily rhythms go on to become the underpinnings of a cardiac care regimen that may offer treatment alternatives that can save a life. The clinicians go on to new patients and new rhythms and new reports. But each person who wears a monitor is brought to bear the feelings of their own life force beating in his or her chest sometimes wildly out of control. For those with irregular heart beats it can be 30 days of fear, impending doom, and personal paroxysm that seems to go on forever as skipping beats and palpating rhythms. And even those with a normal EKG, the fear and worry of not feeling well can be just as agonizing as the beats are uploaded one at a time with not so much as a “job well done” and encouragement to call again tomorrow.
The fundamental appetence for living is shaped by the relationships made during life. Those relationships that nurture and sustain may extend ones years of viability. Some believe the force of life is the beating heart. For without a healthy heart the quality of life may become desultory and life itself may become nothing more than a daily upload of irregular beats on the telephone, in real time.
ROAD MAP TO VIOLENCE – WHAT CAN WE DO TO PREDICT VIOLENCE?
There is no single road map to understanding the complexity of human behavior in general and homicide in particular. If there were the rate of domestic violence homicide might be reduced to zero. Unfortunately behavioral analysis as a science has not evolved into a reliable enough predictor of murder and cannot envisage when terminal rage might be unleashed. The psychological autopsy is the study of individual cases that uncovers details about the pre-incident behaviors known as red flags. The application of this information can identify commonalities among cases of domestic violence so that police and social service agencies might have justification for early stopping and when necessary containment of high risk abusers.
 ne that is safe and prosperous. I expect that most people wish others peace and prosperity on New Years Day.
ne that is safe and prosperous. I expect that most people wish others peace and prosperity on New Years Day. As early as 1984, I served the pediatric population in Boston at the Boston City Hospital Pediatric Emergency Department as the on-call clinician in psychology. That same year I was appointed to the ED at Hale Hospital in Haverhill, MA for screening people in crisis. Those who were stable and had support systems in place would be released – usually with an outpatient referral. Meanwhile, patients without at-home safe guards who could not plausibly answer the question “what brought you to the decision to harm yourself?” were admitted to the hospital. Other mitigating factors like healthy living arrangements, employment, sobriety, and no history of suicidal behavior were positive indicators of future outcome. It was a position I loved and is an important clinical role to this day across the United States. Later as a community mental health psychologist in Long Beach, CA, I served the Children’s Service as someone charged with screening adolescents in crisis living across Los Angeles County. In each of these locations I worked closely with social workers, case managers, police and gatekeepers at state and county psychiatric units to find open beds for kids in need.
As early as 1984, I served the pediatric population in Boston at the Boston City Hospital Pediatric Emergency Department as the on-call clinician in psychology. That same year I was appointed to the ED at Hale Hospital in Haverhill, MA for screening people in crisis. Those who were stable and had support systems in place would be released – usually with an outpatient referral. Meanwhile, patients without at-home safe guards who could not plausibly answer the question “what brought you to the decision to harm yourself?” were admitted to the hospital. Other mitigating factors like healthy living arrangements, employment, sobriety, and no history of suicidal behavior were positive indicators of future outcome. It was a position I loved and is an important clinical role to this day across the United States. Later as a community mental health psychologist in Long Beach, CA, I served the Children’s Service as someone charged with screening adolescents in crisis living across Los Angeles County. In each of these locations I worked closely with social workers, case managers, police and gatekeepers at state and county psychiatric units to find open beds for kids in need.