San Antonio, TX – February 25, 2017 Police officers wear many hats these days. I have spent the last few days learning about a specialized police unit in San Antonio Texas with the SAPD. The Mental Health Unit is a small, well-trained group of police officers who have committed themselves to the positive interaction of police officers and citizens with presumed mental illness. These police officers have a unique window into the chaos some families experience and the opportunity to bring calm to crisis (Sefton, 2014). In many cases, the correct response to this dysfunction should include a follow-up visit in the aftermath of the initial call when the dust has settled from the crisis that brought police to this threshold. When this is done it establishes a baseline of trust, empathy, and resilience. It works and I have seen it for myself.
Over a 15 year span the SAPD has established relationships and built a continuum of service whose mission is jail diversion and treatment for those who are afflicted with mental illness and substance abuse. The Restoration Center in downtown San Antonio is the nucleus for this “smart justice” model. It includes a mobile crisis outreach, 48 hour hospitalization, if necessary, a 90-day homeless shelter with job training e.g. resume building and job interview clothing, childcare and apartment units for those who qualify. As subjects move through the continuum they are provided referrals for individual psychotherapy, substance abuse education, Alcoholic’s Anonymous and the range of 12-step recovery programs. And everyone working there buys in.
Police are the front line responders to crises of all kinds. Asking them to serve in this new role presents a level of officer specialization like never before. Michael Sefton blog post 2013

I was given the complete tour and introduced to some key players including Ms. Amanda Miller coordinator at the Mobile Outreach program. The experience was enriching and illustrated the range of possibilities of humane care for those most vulnerable and often incompetent to make healthy choices for themselves. I wasn’t sure what to expect but I came away wishing I could have stayed on longer. The project diverts citizens into treatment in lieu of incarceration and also serves as an in-house resource where brother officers can turn when times get tough. And the mental health unit has seen its share of despair and self-destruction on their side of the blue line with sometimes insufferable results.
Police officers’ department-wide are trained in techniques of crisis intervention by the same two officers I was fortunate enough to ride with. For years, too many emotionally troubled citizens wound up among the incarcerated criminal population in state and county jails and did not receive the care they needed. In Bexar County, Texas, which includes San Antonio, with a growing population of over 1.5 million the main jail now has 800 open beds where it was once filled to capacity.
San Antonio and over 22 communities share the services of the Restoration Center in downtown San Antonio
Culpability and Mental Illness
Are those with mental illness culpable for their behavior? Technically they are responsible unless determined to be unable to discern right from wrong based upon their mental incapacity. Does the fact that they suffer with conditions like bipolar depression, schizophrenia, or drug addiction render them not responsible? There is a national trend to view those with active mental illness as “not responsible” for their behavior largely due to the common belief that if the mental illness were being treated than the criminality in which they may be embroiled would plausibly diminish. Whenever something sensational happens like a school shooting or some other senseless criminal act people universally remark “he was sick” or “she must have been out of her mind” to do that. Not so fast say the social scientists where as the true prevalence of diminished capacity is quite rare.
I strongly believe that mental illness does not exempt citizens from responsibility for crimes they commit. I agree that alternative sentencing may be a powerful tool to bring these individuals into treatment. The substantive goal of streamlining encounters between police officers and citizens who suffer with untreated emotional problems belies the mission of these gifted officers and can teach others the role of discretion in mental health encounters. The reason for this is to deescalate potential violence and thereby reduce the incidence mentally disturbed persons who wind up in jail. This speaks to the importance of getting those most in need into treatment and off the streets sometimes by having a judge mandate they enter treatment. When charges are brought forth alternative sentencing models may offer leverage that include mandated treatment in lieu of jail time know as alternative sentencing. Studies show that those who remain in treatment are less violent than those who fail or drop out of treatment, Torrey, et.al., 2008. In Massachusetts where I served as a police officer for 12 years too many myths entangled the process of accessing treatment for the mentally ill. Officers were sometimes unsure of their options when a Q-5 prisoner was brought it and rarely made referrals for mental health care. Q-5 is the nomenclature used when referring to someone with a history of mental health issues – usually suicidal threats. These prisoners were required to be on one to one supervision when held in jail. At least that was the myth at the time I was serving.
Community Policing and Aftermath Intervention

I learned several important things about police officer interaction with citizens having mental illness. It is a complex and time consuming endeavor that requires follow up in the aftermath of a crisis. Police officers build credibility and trust in the process of this community interaction with citizens and those in the treatment continuum like physician Roberto Jimenez, M.D., a psychiatrist who has been there from the beginning in Bexar County. Dr. Jiminez began his career in Boston at the once revered Boston City Hospital where I completed my postdoctoral fellowship. He said to me “we had the national model in Boston….” referring to the system in place for police-mental health interaction in 1980. At the time, his service was utilized in conjunction with the state department of mental health and an active system of neighborhood health centers throughout the city. He referred to himself as the police psychiatrist. By then, the Massachusetts state hospital system had been deconstructed and was no longer in the continuum of care. The chronically ill fell off the treatment radar. Importantly in Massachusetts, this triggered the swing away from hospital-based care to the community health centers who became the front line for those in crisis. At this point the myth of mental illness began its insidious transformation. Jail became the containment locale in the absence of the venerable state hospitals for better or for worse. In January 2017, Massachusetts Governor Charlie Baker expanded number of available beds at the Bridgewater State Hospital for care of those in crisis.
Officers in the SAPD Mental Health Unit undergo specialized training in crisis intervention. Officers Stevens and Smarro teach the 40-hours class to police officers from across the country. All police recruits in the SAPD academy are given this training as part of their early law enforcement education suggesting strong support from the command hierarchy. Importantly, the CIT model teaches officers to return to the scene of their calls to make referrals for care as I observed in February. The follow-up call is key in rebuilding trust and illustrates the commitment in police-mental health care continuum. Just as importantly is the relationship created among police officers and direct service personnel like Dr. Jimenez who share the understanding of what can be done for those most in need.
Ostensibly, building relationships with network psychotherapists, physicians, addiction specialists, court judges, and other support service like Child and Family Services is essential. Officers Stevens and Smarro spent hours on the telephone reaching out to the network of physicians, judges, hospital admission personnel and brother officers all in the service of a single case they picked up one evening while on an overtime patrol shift. Had they not caught the call on that night the complainant family may have flown under the law enforcement radar forever and a 33-year old depressed and delusional male may have become increasingly morose perhaps violent. Instead he was put into treatment with the real eventual possibility of receiving social security disability payments to help he and his family and the treatment he needs to begin life again. Next is a strong conviction in what you are being asked to do. It is necessary and constitutive work that often flies below the radar and out of the headlines. It requires patience, flexibility and the right temperament. And finally, officers need to follow-up on calls and build bridges and trust with those they serve including members on the same side of the thin blue line.
Setting the San Antonio program apart is the routine followup in the aftermath of high intensity calls such as domestic conflict or the run-of-the mill calls to houses where families are struggling with under employment, substance use or any number of social problems. A brief second or third visit may just do the trick to hook in a family or individual otherwise in the margins of society bringing forth growth and human contact.
REFERENCES
Perry, D. 2016. Changing the way police respond to mental illness. http://www.cnn.com/2015/07/06/health/police-mental-health-training/
Sefton, M. 2014 Aftermath Intervention: Police first to the threshold. https://wordpress.com/post/msefton.wordpress.com/599
Sefton, M. 2017 Police as therapist: the inherent risk of unconditional positive regard. Blog post. https://msefton.wordpress.com/2017/01/16/
Torrey, CF et. al. 2008. The MacArthur violence risk assessment study revisited: Two views ten years after its initial publication. Psychiatric Services, vol. 59, issue 2, February 2008, pp. 147-152.

")
 As early as 1984, I served the pediatric population in Boston at the Boston City Hospital Pediatric Emergency Department as the on-call clinician in psychology. That same year I was appointed to the ED at Hale Hospital in Haverhill, MA for screening people in crisis. Those who were stable and had support systems in place would be released – usually with an outpatient referral. Meanwhile, patients without at-home safe guards who could not plausibly answer the question “what brought you to the decision to harm yourself?” were admitted to the hospital. Other mitigating factors like healthy living arrangements, employment, sobriety, and no history of suicidal behavior were positive indicators of future outcome. It was a position I loved and is an important clinical role to this day across the United States. Later as a community mental health psychologist in Long Beach, CA, I served the Children’s Service as someone charged with screening adolescents in crisis living across Los Angeles County. In each of these locations I worked closely with social workers, case managers, police and gatekeepers at state and county psychiatric units to find open beds for kids in need.
As early as 1984, I served the pediatric population in Boston at the Boston City Hospital Pediatric Emergency Department as the on-call clinician in psychology. That same year I was appointed to the ED at Hale Hospital in Haverhill, MA for screening people in crisis. Those who were stable and had support systems in place would be released – usually with an outpatient referral. Meanwhile, patients without at-home safe guards who could not plausibly answer the question “what brought you to the decision to harm yourself?” were admitted to the hospital. Other mitigating factors like healthy living arrangements, employment, sobriety, and no history of suicidal behavior were positive indicators of future outcome. It was a position I loved and is an important clinical role to this day across the United States. Later as a community mental health psychologist in Long Beach, CA, I served the Children’s Service as someone charged with screening adolescents in crisis living across Los Angeles County. In each of these locations I worked closely with social workers, case managers, police and gatekeepers at state and county psychiatric units to find open beds for kids in need.
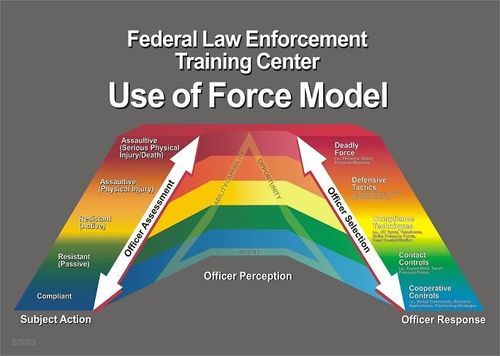
 The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.
The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.