WESTBOROUGH, MA August 22, 2015 The call for police training in de-escalation for persons who are menacing with guns, knives, or bombs is patently unattainable and wantonly dangerous to everyone. Those who call for “more training in mental health counseling and less training in the use of firearms” or use of force continuum have never been faced with the life or death conundrum – kill or be killed. The split second it takes to respond to a threat in defense of oneself or another person will not permit time to introduce strategies for de-escalation. In the time it takes to find ‘just the right words’ to engage the subject who is waving a firearm and shouting that “anyone who comes close will be shot,” people will die – including members of the police who are trained and responsible for calls like this. That being said, the use of force continuum serves as a template upon which police officers first judge their response to calls for service. Officers are trained to give clear commands that are geared toward de-escalating the scenario with a goal of compliance. If the subjects complies with officer commands there will be no force utilized or needed to end a high risk call such as the one described.
PHOTO (AP Photo/Mark Lennihan)
People are asking for added training for law enforcement personnel in mental health awareness. Those individuals wrongly believe that having better “people” skills will reduce the number of officer involved shootings. It is incumbent on society – not the police service to provide care for those who are mentally ill. Unfortunately, there are too few options for those suffering with emotional affliction. It does not matter that Mr. Jones is depressed over an impending divorce if he is engaged in lethal violence toward his wife and children. Once the threat of armed violence is reduced or eliminated when Jones is taken into custody than police officers can offer a sympathetic ear and refer him for psychotherapy – something he surely needs.
The essential element in officer involved shootings is noncompliance to police commands by the subject of police scrutiny. It is the actions of the subject that direct officer behavior. If those actions are coupled with the threat of imminent, life threatening harm only then is a law enforcement officer justified in using lethal force. As long as that threat exists, no one is safe and police officers must adhere to the established use of force continuum that allows for the use of lethal force when an officer is met with the threat of lethal violence.
The incidence of violence against the police is far greater than police acting violently against a citizen. Ask any police officer and they will tell you that police encounter menacing and violent citizens on a daily basis and rarely are required to use lethal violence. Why? Most officers are already highly skilled at using their verbal skills to de-escalate a violent perpetrator without using lethal force – even when a higher level of force may have been warranted. Excessive alcohol and drug use coupled with the lack of clinical infrastructure to provide treatment are the underpinnings of violence – especially in the setting of unemployment and abject poverty.
WESTBOROUGH,MA July 1, 2015 As the analysis of officer involved shootings gradually becomes clear it becomes inevitable that people begin to wonder about the cumulative number of victims of these shootings who may be diagnosed with some form of mental illness. When it comes right down to it the fact that these persons may or may not of been a victim of unjustified police officer involved shootings will be evaluated on an individual basis based on the use of force continuum to which all police officers adhere. “The underpinnings of violence are often present in some form or another whether or not someone has a mental illness ” according to Michael Sefton, Director of Psychological Services at Whittier Rehabilitation Hospital in Westborough, MA. Now a groundswell of support has begun for victims of police shootings that may be the result of untreated conditions with psychiatric etiology. Some are calling for advanced training in crisis management as a way of avoiding officer involved shootings of those who may be emotionally distraught. I agree to a point that better police-citizen interactions may reduce the incidence of escalating violence. But this will not work when someone is exhibiting the cognitive confusion and distorted thinking associated with terminal rage.
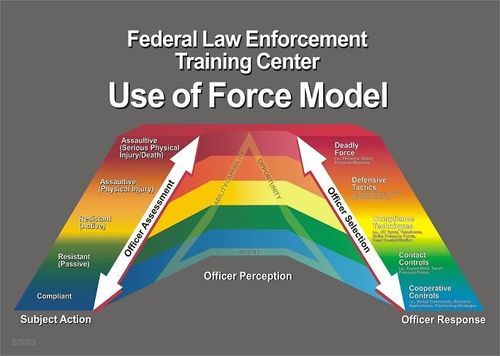
The Use of Force continuum guides officer response to violence and lethal threat
Police officers respond to violent scenes only to face real threats from people who mean to harm them or themselves whether mentally ill or not. To say that it is because they lack training in techniques of crisis de-escalation that some deaths may have been prevented is unfair and short sighted. Lives may have been saved if those individuals purported to have metal illness had chosen not to pick up a weapon and become menacing. Lives may have been saved if those same individuals were not intoxicated or high on drugs when they encountered the police and then became menacing. And again, lives may be saved if there were treatment programs available for those same individuals to provide containment of the most violent, unpredictable and paranoid and psychotherapy for those who might profit from the talking cure. The facts are clear that deadly force was utilized in cases when someone’s life was threatened. Step one of de-escalation training calls for strong voice commands to “put down the weapon”. In cases where these commands were not heeded the use of lethal force may be a last resort.
Police officers are called upon to use deadly force in the protection of themselves of someone else. Training and experience kick in when violent intentions are directed at police officers who are expected to protect potential victims from violence. But yelling and pointing guns is “like pouring gasoline on a fire when you do that with the mentally ill,” said Ron Honberg, policy director with the National Alliance on Mental Illness cited in the Washington Post article on July 1. Mr. Honberg fails to realize that if officers are yelling and pointing firearms it is because the force continuum has already exceeded the level of a shoot-don’t shoot lethal force scenario. The degree of response intensity follows an expected path that is based on the actions of the perpetrator not the actions of the police. The Post integrated video clips from officer involved shootings and the Longview, TX incident depicts how quickly someone with a knife can cover the distance between two officers. Read my published blog on the Myth of Mental Illness as it cites the truly low incidence of crime and violence among those diagnosed with mental illness. (https://msefton.wordpress.com/2015/03/02/the-myth-of-mental-illness-and-school-violence/)
The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.
In a published a blog I have reported that mentally ill persons are no more likely to be violent than individuals without mental illness. However, individuals exhibiting paranoia and those with the acute suicidal ideation are at high risk for acting out violently against police officers and engaging in “suicide by cop” behaviors and place them at greater risk for having lethal force being used against them. There are no single words that will de-escalate someone who has decided on killing themselves or someone else. More importantly, the dynamics of the suicide by cop scenario are a lose-lose for everyone involved – except perhaps the suicidal person who gets what he wants.
“Nationwide, police have shot and killed 124 people this year who were in the throes of mental or emotional crisis, according to a Washington Post analysis. The dead account for a quarter of the 462 people shot to death by police in the first six months of 2015” (June 30, 2105). This is but a fraction of the number of persons who experience suicidal ideation on a daily basis who do not act out their behavior in such a destruction manner. Published accounts have recently blamed the lack of police officer training in managing psychiatric emergencies as a possible underpinning of increased officer involved shootings of persons exhibiting signs of mental illness. Arguably, as a psychologist who has worked with people in crisis, it is often quite difficult to assess who is most at risk for self-destruction because those who are most dangerous often appear quite sane. 2007 Virginia Tech mass murderer Seung-Hui Cho gave off few clues of his grave intentions before killing 32 innocent students – yet the video taped manifesto left no doubt that he was experiencing significant emotional conflict. Ultimately, Cho had been hospitalized at least once for depression and paranoia but was free to purchase the firearms he used on April 16, 2007 culminating with his frenetic shooting spree and suicide.
In Los Angeles, CA the police have an active mental health response team that assist police officers on scene by “slowing things down” using trained, persuasive negotiation in an effort to defuse high stress incidents and lower the number of lethal encounters. The program in L.A. seeks greater communication and understanding between the police and members of the mentally ill community, according the the Washington Post. Mary Jo MacArthur is the assistant chief of the L.A. police training program. She teaches that those in crisis do not process information like other persons and may experience fear and anger when given verbal commands they do not understand. The L.A. model provides for professional support from trained psychologists or psychiatrists on scene. But an officer who encounters an impulsive and violent man menacing with a firearm or knife cannot be expected to de-escalate and “slow down” a volatile situation when the threat of lethal force being used against them or someone else exists in real time.
It is inflammatory to say that police did not handle this case or that case appropriately. The use of force continuum is clear that force is met with similar degree of force in order to control and de-escalate. Any other mismatch of force place everyone in grave danger. Once the lethal threat is neutralized – such as when the mentally ill person drops all weapons and submits to verbal commands to surrender – additional investigation and support may be provided by local mental health teams including hospitalization as needed. Another program exists in Vancouver, B.C. that I will review in my next update.
Police officers are regarded as the front line first responders to family conflict and crisis. The most volatile scenes are those where mental illness coexists with substance abuse like heroin addiction and domestic conflict. For better or worse, the police have an opportunity to effect change whenever they enter into the domestic foray or crisis involving members of the mentally ill community. This affords them a window into the chaos and the opportunity to bring calm to crisis. In past blogs I have introduced the notion of aftermath intervention as a means to ending the repetitive nature of those in crisis. Added training to deconstruct the myths of mental illness after each encounter may be useful but time is seldom provided for such debriefing. As with many states who review domestic violence homicide – mental health response teams based on the L.A. model and post hoc analysis of red flag indicators of the potential for violence fueled by mental illness i.e. delusions, hallucinations, active PTSD, should be carefully crafted for officer and community safety.
“Community policing has long espoused the partnership between police and citizens. The positive benefits of this create bridges between the two that may benefit officers at times of need – including the de facto extra set of eyes when serious crimes are reported” (Sefton, 2013). These extra eyes may be called upon to identify red flags as they wave suggesting someone may be headed down the path of destruction. In the case of some noteworthy domestic violence, post hoc analysis often reveals that people were aware that something was going to happen and not a single person stepped up to strike a warning (Allanach, 2011). Police agencies cannot work in a vacuum and must have the help of citizens if they are to have any impact de-escalating the mentally ill prior to onset of terminal rage.
In many cases, the correct response to intimate partner violence should include aftermath intervention when the crisis has settled from the crisis that brought police to this threshold. Techniques for understanding mental illness may facilitate mutual understanding and establish the needed bridge to facilitate treatment. When this is done it establishes a baseline of trust, empathy, and resilience and may lessen the likelihood of the violent menacing that demands force be met with force regardless of the diagnosis. In the next blog I will identify the role of police officers in pre-incident intervention and identify a chilling case. By the time a person is in crisis there may be little time to talk “sense” and de-escalate no matter how skilled and well trained the police become.
REFERENCES
Ronald Allanach et al., Psychological Autopsy of June 13, 2011, Dexter, Maine Domestic Violence Homicides and Suicide: Final Report 39 (Nov.28,2011), http://pinetreewatchdog.org/files/2011/12/Dexter-DVH-Psychological-Autopsy-Final-Report-112811-111.pdf
Sefton, M. (2013) Blog: Aftermath Intervention: Police first to the threshhold. December 8, 2013 Taken June 30, 2015, https://www.msefton.wordpress.com/2013/12/08/aftermath-intervention-police-first-to-the-threshold/
It is time to look at the impact of digital connectivity
WESTBOROUGH, MA January 12, 2014 Elevated stress and tension are sometimes the price of technology. When human beings become fixated with having all the updated information there becomes an overload of sensory stimuli including images, text and integrated multimedia. In times of national emergency people stay connected to sources of information like CNN, the Washington Post, or other national media source. Arguably, this can save our lives and bring us valuable information and needed instruction at times of national crisis. At the same time, the tethered tie to technology reinforces adrenaline junkies like never before.
Prior to culmination of last years terror attacks in Boston, readers and television viewers alike may have been glued to their internet devices waiting on every new post of information. Meanwhile thousands of people took to the twitter feeds and other social media to post their impressions and notify the world that their tiny digit footprint was alive and well in cyberspace and on the ground. All the while, they white knuckle their smart phones posting and tweeting with hope of reaching someone who might regard their importance and be mindful. Unfortunately, there is a price to be paid when this type of sensational event occurs. The human body reacts each time a flurry of tweets is released with alarm, threat, grief, and satisfaction. The human interpretation of these stimuli have the power to create dramatic physiologic changes in the autonomic nervous system. These lead to insidious, heightened autonomic arousal, increased blood pressure, anxiety and perhaps burn out.
Pavlov had it correct when he described how rewards shape human functioning and how frustrated animals become neurotic trying to gain some fickle reward. Behavior is molded through a series of subtle reward and punishment protocols. Rewards result in an increase in behavior. Punishment will cause a behavior to become less frequent and eventually extinguished. In 2014, the ‘need to know’ is rewarded by having immediate access to information. This is a good thing. Web sites that falter or offer old news are forsaken for the more instantaneous text and images – like old magazines. Media outlets have taken to social media to access this demand by offering immutable news snippets in the form of tweets or other posts. If this information is accurate and reliable people will listen (or read) in great numbers. But this can go too far when people overdose on social media. For a variety of health reasons it is often a good idea to turn off your digital ping and allow yourself some old fashion quiet. Relaxation is something that comes when the body quiets itself and slowly resets the baseline axis of rest.
The fight/flight mechanism that keeps us on guard plays a primary role on how people feel after episodes of high stress. Feelings of frustration, lack of focus, chronic fatigue, and even depression can result from an over reliance social media stimuli like an unfed addiction. Each time information about the Boston Marathon bombing was released people began filtering a barrage of data being generated – some reliable and accurate and some distorted and confabulated. How many times did we refresh the screen on our smart phones only to see that same header and feel frustrated or angry at the snail’s pace of new information?
People asked “what should we tell the children” when referring to the bomb blasts in Boston. Television had taken over the airwaves with live broadcasts. For several days before the capture of Dzhokhar Tsarnaev the Boston metropolitan area was closed down making it seem like a ghost town. Massachusetts Governor Duval Patrick asked for a voluntary closing of business including the shut down of public transit, buses and trains. People began to feel the loss of freedom so common in other places on the globe like the West Bank, South Sudan, and now Syria where people live in perpetual fear of violence, torture, and persecution. But this was occurring on U.S. soil in a vibrant city on a day where thousands of visitors were running a race for as many causes as you can realize – and perhaps some personal cause of freedom.
Experts finally agreed that the best response would be to turn off the television and allow kids to process what they may have seen. There come’s a time when the technology begins to overwhelm. Too much stimuli results in the over abundance of stress hormones that can trigger physical discomfort and interfere with sleep, cardiac rhythms, mood, and needed rest.
The long-term consequence of technology is unclear. The human cost is measurable in terms of information overload and digital dump. Some believe our brains adapt to the instant gratification of social media and develop a graving for the deluge of tweeted stimuli or some instagramed image. Slowly, the body learns to habituate the barrage of stimuli selecting only that which is most novel or unique using a form of cognitive triage. In the process of habituation people seek more and more stimuli to raise the digital threshold for avoiding boredom, stagnation, and falling prey to yesterday’s news.
People who grow up in war zones demonstrate a similar malfunction in their system of arousal marred by hyper vigilance due to perpetually imploding stress hormones. This is the result of chronic exposure to unpredictable chaos and the stress associated with a lack of control. Neuroscientists can now pinpoint the impact of stress on hardwired changes in the brains of children growing up in places without lasting peace. Social scientists attribute similar developmental mechanisms to the cognitive behavioral underpinnings of children exposed to severe domestic violence. Stress has undeniable impact on all human functioning and public health. Not enough is being done to infuse knowledge and understanding into the emotional Molotov created by chronic stress. Why would healthy people create an unhealthy lifestyle in the absence of uncontrolled calamity? If the dynamic of 24/7 connectivity adds to our health woes than its seems intuitive that we would cut down on our hunger for apps and need for the unending adrenaline dump created by this technology.
What will become of quiet space, solitude, and the capacity to be alone? There is nothing more irksome than someone walking through a grocery store while chatting on a cellular phone as if she were alone in a comfortable study – laughing, telling personal stories, perhaps arguing with a detached spouse. As much as I glare at that person – willing them to choke on the gum they seem compelled to chew, they seem totally oblivious of my overt distaste for them. This person can not be alone even for the time it takes to procure items for the nightly supper or the few needed toiletries for an upcoming trip about which we shoppers heard tell.
To be alone and to experience alonness is a healthy function. The loneliness felt by many can drive the unquenching thirst for data, information, and the pseudoconnection that comes with a digital age and the feelings of angst at not getting pinged.
WESTBOROUGH, MA May 24, 2015 It’s time I write a paper about the role of heroin on addiction and the dramatic rise in overdose-related deaths. More needs to be done for people addicted to heroin. The town in which I live has had three or four young adults die from heroin in the past 12-24 months. These were real life people who went to school with my children and could be seen in the sports pages excelling on the field of play. They were high school graduates from great families. They were attending college. They had homes or apartments to live in. They had names and faces.
There is no shortage of stock photos available to depict this scourge. Each of them leaves me feeling sick.
Heroin addiction is a gripping, life suck that robs and maims anyone who uses it. I am a psychologist but make no claims about helping those suffering from the physical and emotional gird of heroin. There is no bottom to the cycle of addiction for many individuals and their families who often spend a fortune on psychotherapy, rehabilitation programs, 12-step programs, and nasal naloxone. Most individuals trying to kick the heroin habit require 4 or more trips to rehabilitation.
This is the story about Netta and the boy who grew addicted to its insidious lure. Netta was a term given to heroin or more specifically, the nick name for “the works”. This refers to the needle, spoon, filter, and lighter used to inject heroin into the vein by someone wanting to party. There can be no party without the works and this boy kept his immaculate. This addict strangely personified his rig as a friend or more importantly, a friend who could bring forth comfort and a rush of euphoria that nothing else can match. He was not one to share needles with others and most often used when alone. He also knew this friend could not be trusted and expected to die one day perhaps ironically after deciding to get clean and sober. An overdose can take you to the grave and has done so with a vengeance in 2015 here in Massachusetts and across the country. The man about whom I am writing died recently of an overdose that some believe was intentional. He had grown tired of the cycle of addiction and pain and sickness. He died alone.
For many addicted to heroin saying ‘no’ is not an option and becomes a game of Russian Roulette. It does not matter to Netta whether or not you are rich or poor he will take you for all you have. He will leave you numb and sick and looking at cotton shots for just a little more. In many states like Massachusetts, police, fire and other fire responders have been trained to administer nasal naloxone. Arguably, family members too should be given the antidote which can reverse the effects of heroin and other opioid drugs if administered soon enough. That is where the confusion comes in because while naloxone can reverse or eliminate the effects of opioids in the brain it cannot reverse the cascade of organ failure and brain injury associated with oxygen deprivation.
There needs to be some intervention that can help individuals addicted to heroin and more importantly to help them when the urge to party comes up over and over during recovery. There should be support for their family members so that they might understand the allure and better connect with those who are living a life with friends like Netta.
This blog was initially published in March 2013 as a retrospective on the recent spate of “active shooter” tragedies across America. There have been several high-profile shootings in the past 3 years that have involved perpetrators whose mental health is in question. This is often not the case in school violence whereas the perpetrator of the action was deceased at the conclusion of the incident. In these cases an effort must be made to uncover substantive causal factors in the perpetrator’s terminal actions.
The true incidence of violence among people diagnosed with a nervous and mental disorder is quite low. It is a common misconception that whenever something hideous occurs it must be mental illness that is the driving force behind its fury. In most cases this is neither the reality nor the underlying cause of terminal rage. In light of the information being uncovered about the Newtown, CT mass murderer, the specter of mental illness insures a convenient scapegoat. Updated information from Newtown recently confirmed that Adam Lanza had studied the media stories of prior mass killings as he planned for his despicable final melt down. In retrospect, I wonder what “red flags” have been uncovered that offer insight into his substantive motivation. People will speculate about random causes of Lanza’s behavior with uncertainty unless it can be studied scientifically.
There are some instances when mental illness has be associated with serial homicide such as the Son of Sam killer who plied his murderous delusions in NYC during the 1970’s using a Charter Arm’s Bulldog .44 caliber revolver. David Berkowitz used that weapon to kill 6 and wound 7 during his spree. He claimed to have been commanded to kill random couples he saw in cars by a dog he believed possessed by the demon. After spending time in a mental institution following his conviction he was transferred to the state prison at Sing Sing and finally Attica to serve 6 life sentences. When he was on trial Berkowitz plead not guilty by reason of insanity – the delusions he had about communicating with demons. In the end, it was determined that Berkowitz was not mentally ill. The Columbine, CO high school killers, Klebold and Harris were methodical in their planning of the attacks on the school and its students. They built explosive devices and practiced their attack in the weeks before the assault on the school. By outward appearances these two were from middle class families with involved parents. Many believe Klebold and Harris were the victim of bullies.
Psychological experts believe mentally ill persons lack the higher order planning to execute the complex steps necessary for these types of crimes. Neither Dan Klebold nor Eric Harris was mentally ill. The Virginia Tech killer Seung-Hui Cho murdered 31 students and faculty in 2007 after a period of decompensating rage. He wrote a profanity laden manifesto blaming everyone for their maltreatment of him that sounded paranoid and vindictive yet was able to send the videotaped diatribe to a news agency. Cho had been held in a psychiatric hospital 2 years prior to his rampage after becoming marginalized. Cho was able to organize his crime preparation and sequence the needed steps to meet his murderous goal. Was he mentally ill?
The Psychological Autopsy is a clinical assessment of the time line and antemortem behavior and emotional comportment of the perpetrator of compelling and despicable events. These types of case studies explore changes in cognitive and behavioral functioning immediately before a terminal event of homicide. An extensive review of a case from 2010 that was published in 2011 generated over 50 recommendations about DV and factors to consider when victims are at greatest risk (Allanach, R., 2011). The cost of these interviews and substantive case review is the primary reason they are not regularly conducted. It is also less compelling when the perpetrator has killed himself and survivors want to turn the page.
Recently, at least 2 shooters have survived mass killings or have been captured after their alleged attacks. In 2012 in Aurora, CO movie theater James Holmes was arrested and charged with multiple counts of murder. He has pleaded not guilty by reason of insanity. In 2011, Jared Lee Loughner was arrested at an outdoor political event in Tuscon, AZ after the shooting of U.S. Representative Gabrielle Giffords and killing 6 others. Loughner plead guilty after being found that he was capable of standing trial.He is serving 140 years in prison. The Aurora case remains open.
It is hoped that important information may be gleaned from the rigorous study of motives, personal history, and triggers to their rage.
REFERENCES
Ronald Allanach et al., Psychological Autopsy of June 13, 2011, Dexter, Maine Domestic Violence Homicides and Suicide: Final Report 39 (Nov.28,2011), http://pinetreewatchdog.org/files/2011/12/Dexter-DVH-Psychological-Autopsy-Final-Report-112811-111.pdf.
Sefton, M. (2011) The Psychological Autopsy: Provides a host of pre-incident indicators. Blog: http://www.enddvh.blogspot.com/2011/11/psychological-autopsy.htm, taken May 26, 2014.
WESTBOROUGH, MA January 20, 2015 Dementia is a life changing affliction for both the patient suffering with the neurocognitive decline and spouse and family members alike. Caregivers have a particular cross to bear – especially those without support. It is a highly stressful role for any spouse that requires both education and support. They are at high risk for burnout otherwise known as caregiver fatigue. For anyone who has had a loved one suffer with this disease “it is like seeing a family member die slowly, daily, withering away into an empty vessel” according to Michael Sefton, Ph.D., Director of Neuropsychology at Whittier Rehabilitation Hospital in Westborough, MA. “It is very important to obtain a careful and sound neuropsychological assessment of patients’ suspected of having dementia because so many conditions mimic dementia and may be treatable” according to Sefton.
When a caregiver is overwhelmed something must be done to provide emotional respite for the spouse or family member. Caregiving spouses frequently have powerful feelings of guilt, anger, and sadness as a result of seeing a loved one become forgetful, detached, and confused. They can be extremely difficult to managed in the home setting and sometimes require specialized day treatment. The decision to hospitalize or seek nursing home admission for a family member is an individual one. It is critical to look at the functional change in the afflicted family member and see what placement options make the most sense. Caregiver fatigue places afflicted patients at greater risk for neglect, battery and abuse than other medically complex cases. It places caregivers at risk for health problems of their own.
Throughout America, physicians and psychologist alike are mandated reporters for cases of suspected abuse – regardless of whether the caregiver is experiencing caregiver fatigue or not. Family members are strongly encouraged to support parents, e.g. respite care for afflicted parent, whenever one is suffering from a severe illness like dementia. Read the post at link below.
Lena told me she grew up in East Germany – behind the iron curtain from which she escaped when she was 33. Her best memories were from a time when Hindenburg was the country’s president. She lived in East Prussia near the Polish-Lithuanian border where most East Germans were Lutheran. As children, they were made to stand under the “Hitler cross” each day before school and recite the Socialist pledge for nationalism that she cannot forget. She recites the narrative for me in her native German – translating the final few words into English – “the flag is more important than the dead” she mocked shaking her head. Lena had an unexpected and compelling history about which her doctors seemed unaware.
They were driven from their homes by the advancing Red Army during WW II in the 1940’s as millions were. Yet, these East Germans were subjected to despicable atrocities most people are not aware of during the evacuation. “They took our homes. The banks were all closed. We had nothing” becoming tearful. I bear witness to Lena’s personal memories – the narrative of her life living under the Hitler cross and the journey to America.
Now 91, she lives alone since her husband died over a decade ago. She lives 70 miles from her daughter. I was asked to interview Lena and determine if she was capable of returning to her home alone after she sustained a fall and broke her humerus – the long bone in her arm. It was the second time she had fallen in the past year. I reviewed the chart and her nurse commented that she is noncompliant and suspicious somewhat randomly. It was my role to provide an understanding of Lena’s cognitive status for the treatment team with some pithy explanation as to why she keeps falling and whether she can go home again.
Lena is frail in appearance and has a small frame. Her eyes are hard and I cannot tell what color they are. Her white hair is wispy, thinning. She is sporting a blue sling that keeps her shoulder from moving. It is her dominant arm I note with some reluctance. Sadly, I wonder if the traumatic recitation I am now hearing may be a sign of the psychic unraveling that some elderly trauma survivors experience shortly before death.
As a consultant I try to remain dispassionate. I need to determine her orientation, awareness of illness, capacity to concentrate, and review her gait training, balance, and daily carry over. I find Lena hard to redirect but I need to respect the urgency of her thoughts while she painfully unburdened herself. I am not optimistic about her returning home.
Moments of pleasure
Lena wants to go home so she can maintain her small garden in which she plants tomatoes and colorful flowers each year. “People admire my yard and sometimes stop to take pictures of the flowers” she reports with a slight and hopeful smile. She even boasted a one-handed technique used to plant her garden last year after suffering a shoulder injury in her first fall. With her left arm she dredged an orifice just large enough for the seedling. Then with the heel of her foot she covered and packed the plant with great acumen and apparently admirable results. Resourceful and independent, I thought bringing new meaning to the green thumb adage.
Unfortunately for Lena, there is more than just making her garden she worries about. She is afraid about what might happen to her home when she isn’t there. There has been vandalism – “they painted the Hitler cross on my mailbox and house and broke my windows” she reported indignantly. “What can you do” her voice trailing off. Once, she paid some boys to shovel the driveway. They convinced her to pay them before the job was done and ran off taking her twenty dollars leaving only the snow behind. The same thing happened with the landscapers who she had hired to rake the leaves this fall. Can she go home again? I could derive little experience of joy in her history – often an outward sign of depression.
Lena was raised on a farm, I learned. But she had a brief childhood marred by atrocity and abject savagery. She was one of 9 children. “We had horses and cows and an orchard” she reminisced. Lena was brought up Lutheran but had Jewish ancestry. “Her mother was very religious” she described. Because they had property, landowners were expected to attend regular community meetings during which her father often spoke out against the government – against Hitler. “They had an eye on him when he came home from the war” she reflected. “They came and beat him up once, she remembered – somebody told on him” referring to the time he spoke out against the war at the community meeting. His battered and bruised body “looked like a rainbow” when describing his wounds. “Hitler did not grow up a German – he moved from Austria and promised to spread the ‘German way of life around the world'” she mused. “All he did was invent the autobahn”, now her bitterness and mistrust began to show.
Traumatic Losses
Lena saw 15 members of her immediate family murdered. Her father was shot to death in the orchard behind the family home when she was 9 years old by the German secret police because he spoke out against Hitler at a local meeting of property owners. Her 7-year old brother was made to watch. Her 4 older brothers were conscripts and died in the war. Lena said that her grandmother married a Jew. He was very nice, she pleaded. Later, the family home was taken from them and the animals were killed during the evacuation of East Prussia late in the war. By then she had already lost her parents. Neither the Germans nor the Russians were humane to the native population of Lutherans and Catholics, and Jews.
After being forced from their farm, Lena was committed to a warehouse to live. It was one big room. She was made to sleep between similarly damaged souls – many who succumbed – leaving their postmortem remains for others to see. She and her sisters were raped. Elderly women were raped and murdered. “People don’t know” she grieved now bearing witness to spectacles no person should ever see. She described the dreams she has to this day – of being trapped in a room with no escape but would go no further.
I return the next day to see what carryover she has of our first emotional conversation. I notice Lena sitting next to others in the community room – intrepid – yielding no outward sign of her inner torment. She spoke to no one with a glower on her face that could dissuade even the most confident salesman. She nodded and smiled slightly – faint recognition, I predicted. Uncertain. We agreed to meet again later in the day after bingo. I had been strongly impacted by her disclosure and felt I needed to hear more. What had happened to Lena since coming to America? Was she a member of her community? What kind of life had she built here in New England?
The promise of a better life brought Lena and her husband to America in 1952. She had one daughter. Her Lutheran beliefs taught her the importance of helping others in her community – even neighbors on Cape Cod, MA where she still lives. But the efforts made by she and her husband were often not returned in kind. People were not friendly and welcoming so soon after the war.
“My husband was a teacher in a technical school (in East Germany) and used to help the man who lived behind us when his car would not start” boasted the frail woman with a strong German accent. Here she expressed her bitterness at being persecuted by those who were ignorant and prejudice against people who are different – perhaps more so toward immigrants from Germany when they first arrived after WW II. “Kids don’t know about it today” she complained. She worried that the abject trauma she experienced during the second World War would one day become irrelevant – forgotten.
Secondary Trauma
The pain she felt in Germany was not eased by the democratic change of scenery. In fact, Lena herself was accused of killing Jews by a neighbor simply because of her country of origin. Her daughter was bullied and abused between school and home. The child’s principal refused to allow her to come and speak to the students to help them understand that she too had Jewish blood and had suffered unspeakably at the hands of the Nazi’s and those who drove them out. She wanted to protect her only daughter from the hatred and vitriol and suffering she had endured.
“I am responsible for what happens here in school,” said the child’s principal, “not for what happens when she leaves the school grounds” in a despicable collusion of denial and lack of courage. More than anything Lena wanted to shelter her only child from the same truculence she endured and make a better life than the one she knew. She didn’t even know Hitler” she cried, now rocking slightly.
Lena described a time when her husband was burned by acid that had been mixed into the water he used to wash his hands while working a stint in a local automotive garage. Afterward, he was sent to a physician who indicated the condition of his hands was a disease brought with him from their country in an outrageous distortion of the truth.
“You can complain to nobody” she bristled. “The police don’t do anything” she bemoaned. After her home was vandalized, one officer asked “What do you expect us to do sit in the driveway?”
Can Lena go home again? I am sure Lena would love to return to the idyllic family farm with the orchard and horses the way she remembers it before the Hitler cross flew above her school yard. To visit with her large family before the time when her father was murdered and her windows were broken and her mailbox was disgraced with the Hitler cross. Who can you tell, nobody knows what happened anymore?
I cannot envisage a life-like the one Lena has had with its childhood trauma, loss, and recurring prejudice and persecution. Yes, I would expect that Lena is suspicious and mistrustful but she is not paranoid. What would anyone do if they experienced the life events and atrocities experienced by this woman? The emotional resilience Lena has shown raising her daughter and making a home for her family has inspired me to look at her differently than others might have done in my position.
Lena should go home and yet she is at risk of falls when alone. She has fallen and broken both the left and right shoulders – unsteady on her feet. Her fear and anxiety stem from an underlying sense of vulnerability based entirely on her history of personal trauma and abuse while living under the Hitler cross. The reason for her noncompliance and emotional detachment are the predictable product of her early beginning in East Prussia near the border with Poland. It represents her fiercely stout-hearted spirit and enduring strength – features of the emotional veneer that are the underpinning of her being. It would be wrong to remove her from her place of safety and take her from the garden she loves that brings her a few moments of joy each summer. She feels pride in the tomatoes and colorful flowers she has grown for others to stop and see and sometimes even take pictures.
I return yet again to visit Lena and clarify some of her story and see how she is progressing. In what city did she live?How had she coped with the trauma of her life? When I enter her room I notice an aide rounding up the sheets and blankets from her bed. “She has been transferred to a nursing home,” he remarked without emotion. She had been discharged only a few minutes before I arrived. Her doctor believed it was the safest thing to do. Her daughter agreed I suppose.
For whatever reason Lena felt safe enough in my presence to share the narrative of her life over the course of a couple of weeks. I made an effort to deconstruct the mistrust she projected and summarily to lessen her emotional burden. Arguably, I was unable to extract a pithy aphorism that would send her homeward based on my impression. Yet I wanted to explain the rationale for her transfer. I am sure she was dispirited about not going back to the Cape. Again conscripted into battle over personal control and humility forced to sleep once more among the damaged souls. “Nobody knows what happened” Lena might say – but I do now.
“Take care of yourselves, rest as much as you can, read good books, sing loud songs (when you’re alone…would be best) and read a poem now and then”
Personal note in holiday card from Ann Sefton (Mom)
These were the words of Ann Sefton in a Holiday card sent to my wife and I and are among the best advice I have ever received from my mother or anyone else. I think they are worthy and spoken from the heart and I intend to share them with anyone who will listen. The kindness and wisdom in the words struck me as a reminder of the joy and simplicity I seek in my life.
Those words along with the espoused words of David Trimble, Ph.D. are beliefs that foster greater self-awareness, self-compassion, firm authority, integrity, and coherence to my life. Here’s to a great New Year!
Read them and share them with someone you care about.
WESTBOROUGH, MA November 30, 2014 A patient once said Dr. Sefton “don’t ever grow old”. At the time I wondered what he meant. The man was alert, physically fit and had a great support system. We have heard for years that today’s baby boomers are growing older. No kidding, I am one of them. “People believe human touch and the relationships we forge along the way sustain us into our old age with a sense of well-being” according to Michael Sefton, Ph.D., who provides neuropsychological testing for older patients. Along the way the connections we make open our experience and our hearts. As people age, time begins to have greater significance – especially at the end of life. Some people say time moves quicker with age – especially when memory fades. Greater attention to things of importance must include keeping memory and history alive. Ask yourself “what do I value most?” If the answer in your head is money, job promotion, or things like material objects then priorities may be outright misguided. Next, ask yourself how much dignity you might feel if you suddenly were made to feel irrelevant? That is how may older Americans feel as they age and enter the “golden years”. Depression and loneliness are highest among people who are older and have become marginalized. This contributes to the inability to participate in their communities adding to feelings of loneliness and increased risk of functional decline and even early death (Singh, A. and Misra, N., 2009).
Cultures everywhere include senior citizens among the things that are valued and respected although this is not universal. Some believe that with age comes wisdom. Here in America, the population of older citizens will grow by a factor of 2 in the next decade or two. No society should discredit those who are older and may be stepping aside to a younger generation. “Senior citizens, especially those who may be blind, deaf, immobile or senile, contribute less and require more care, which is likely unavailable” according to Discovery Health. The growth of older Americans has far exceed the growth of programs geared to help those in need. Why?
Retirement and aging
For those who are entering the last years of employment a sense of trepidation may confound their decision to retire. The age of retirement has edged upward largely due to financial need. People are constantly speaking out about the need to plan ahead for the retirement years. In a blog I wrote about police officer retirement the success a person feels in retirement depends upon how valued they feel in society (2014). Many believe that older workers are more reliable and bring a higher level of maturity that benefits employers everywhere. Others see the older worker as the greeter at the local box store – someone now irrelevant. The impact of this prejudice adds to a high incidence of depression among people over 65. The rate of poverty among older Americans is greater than 15-20 percent, according to Intergenerational Learning Service based in Illinois. And the rate of grandparent’s who take care of their grandchildren has never been higher. How is this scenario apt to impact human development for years to come?
A fundamental change in attitude must take place toward people who are aging here in America. At the same time, a belief in lifelong learning and personal responsibility for health and well-being will give an older person an equal advantage for those who are aged and wish to continue being relevant.
Michael Sefton
REFERENCES
Singh, A. and Misra, N., (2009). Loneliness, depression and sociability in old age. Industrial Psychiatry Journal, Jan-Jun; 18(1): 51–55.
Terminal rage dissembled by increased red flag threats and violence
WESTBOROUGH, MA November 2, 2014 A group of my colleagues and I were drawn into the chilling events of June 13, 2011 after Stephen Lake killed his family and then himself. During the final moments of his life Lake laid out the death scene ostensibly to torture his spouse from whom he was estranged and ordered to stay away. While police closed in, Lake killed and attempted to burn his victims in an act of emotional mayhem.
Arguably, the murderer in this case became blinded by anger and resentment at perceived disrespect and exclusion from the lives of his children. This anger had grown over the year since a protective order was issued following a violent episode in the family home. The perpetrator grew marginalized during the coming months becoming resentful and humiliated at missing key events like Christmas and an 8th grade commencement. All the while he posted on social media sites his love for his family he grew depressed and disorganized. 12 hours before the violent ending he tearfully described feeling depressed to a family member and was advised to seek help. Lake wrote 9 suicide notes that were found in the days after his death.
Renewed interest in retrospective study
The psychological autopsy revealed an increasing pattern of red flags in the weeks before the murder-suicide in Dexter, Maine. Greater awareness of these red flags may serve as a stopping and containment point for perpetrators of intimate partner violence. In a sad retrospective, the Maine state Chief Medical Examiner cited that “in spite of some mental health treatment the extent of (the perpetrator’s) anger was not fully appreciated”. The research led to a call for no bail holds for some violent abusers and GPS monitoring for others. After 3 years, these recommendations are finally beginning to emerge in the protection of victims of domestic violence in Maine. Mr. Lake was alleged to have violated the protective order more than twice. His reported view of the “cost of divorce was the price of one bullet”.
Who can be expected to bear witness to red flags?
It is well documented that domestic violence is a secret happenstance that effects far too many families across the country. Victims are expected to remain loyal servants of their spouses under the dissembling guise of love and devotion. The findings published in the Dexter, Maine study reveal that people knew what to expect from Mr. Lake. His unwinding was clear to some of his closest family members. A paternal aunt was quoted as saying “I never thought he would take the kids” suggesting an awareness that Lake might kill his spouse and then himself – sparing the children. Others believed Lake might commit suicide in front of his wife and children leaving them with the emotional specter of his violent death. Instead, as the chief medical examiner cited the full extent of Lake’s anger was not appreciated. In this case, as in many other retrospective studies of DVH red flags were not appreciated. Many believe that an order of protection is not effective in protecting victims from violent spouses who seem to ignore “stay away” orders seemingly at will and without consequence. These are the red flags that require containment of the abuser and must serve as the frank evidence of elevated risk for domestic violence homicide.
The team of people helping 22-year old Elliot Rodger, a young man who went on a shooting rampage at the University of California at Santa Barbara in May 2014, all reached out to police and the media when they could not reach the estranged and overwrought man. But they were too late as he had made his mark on history by then. The the Virginia Tech shooting some red flags were missed. Had the subtle clues the Rodger’s underlying mood been recognized the shooting may have been averted. To read the blog from the UCSB shooting click here.
Mandated reporting for domestic violence
As a civilized society there should be mandated reporting for those most at risk for domestic violence and the penultimate DVH as it becomes apparent. Just as practitioners are mandated to report cases of suspected child abuse and elder abuse so too must we begin to take heed of the signs of domestic or intimate partner abuse and take action. By doing this we may save the lives of those most effected by DV and arguably break the recurring cycle of domestic violence. Some people wrongly believe there is nothing that can be done about domestic violence homicide. Others remark that “what happens behind the closed doors in a dysfunctional and violent household is no business of anyone else”. To the extent that this draconian belief system prevails in the public understanding of DVH there is little chance of preventing this scourge. As a result states are slowly changing their response protocols for DV and the police response to signs of abuse with mandated arrest for suspected perpetrators.
Risk assessment of those arrested for domestic violence is often overlooked. However, police departments are teaming up with agencies serving the population of abuse victims like never before and are adopting tools to assess the likelihood of future violence when determining bail amounts. Bail commissioners must be educated about the cycle of abuse and domestic violence when assessing bail amounts. The average abuse victim experiences 5-7 episodes of DV prior to calling the police. Police response to DV has slowly started to include a careful analysis of the history of aggressive events including the number and type of physical assaults that have taken place. Some events are clearly more foreboding like choking to a point of unconsciousness, sexual aggression, threats of suicide, and the use of veiled threats of death if the spouse ever tries to leave. Other behaviors such as unrealistic jealousy may be the underpinning of current or domestic violence. One victim told me that the abuse started as soon as she said “I do” 16 years earlier.
REFERENCES
Ronald Allanach et al., Psychological Autopsy of June 13, 2011, Dexter, Maine Domestic Violence Homicides and Suicide: Final Report 39 (Nov. 28, 2011), http://pinetreewatchdog.org/files/2011/12/Dexter-DVH-Psychological-Autopsy-Final-Report-112811-111.pdf.
Sefton, M. (2011) The Psychological Autopsy: Provides a host of pre-incident indicators. Blog: http://www.enddvh.blogspot.com/2011/11/psychological-autopsy.htm, taken May 26, 2014.

 The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.
The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.



