WESTBOROUGH,MA July 1, 2015 As the analysis of officer involved shootings gradually becomes clear it becomes inevitable that people begin to wonder about the cumulative number of victims of these shootings who may be diagnosed with some form of mental illness. When it comes right down to it the fact that these persons may or may not of been a victim of unjustified police officer involved shootings will be evaluated on an individual basis based on the use of force continuum to which all police officers adhere. “The underpinnings of violence are often present in some form or another whether or not someone has a mental illness ” according to Michael Sefton, Director of Psychological Services at Whittier Rehabilitation Hospital in Westborough, MA. Now a groundswell of support has begun for victims of police shootings that may be the result of untreated conditions with psychiatric etiology. Some are calling for advanced training in crisis management as a way of avoiding officer involved shootings of those who may be emotionally distraught. I agree to a point that better police-citizen interactions may reduce the incidence of escalating violence. But this will not work when someone is exhibiting the cognitive confusion and distorted thinking associated with terminal rage.
Police officers respond to violent scenes only to face real threats from people who mean to harm them or themselves whether mentally ill or not. To say that it is because they lack training in techniques of crisis de-escalation that some deaths may have been prevented is unfair and short sighted. Lives may have been saved if those individuals purported to have metal illness had chosen not to pick up a weapon and become menacing. Lives may have been saved if those same individuals were not intoxicated or high on drugs when they encountered the police and then became menacing. And again, lives may be saved if there were treatment programs available for those same individuals to provide containment of the most violent, unpredictable and paranoid and psychotherapy for those who might profit from the talking cure. The facts are clear that deadly force was utilized in cases when someone’s life was threatened. Step one of de-escalation training calls for strong voice commands to “put down the weapon”. In cases where these commands were not heeded the use of lethal force may be a last resort.
Police officers are called upon to use deadly force in the protection of themselves of someone else. Training and experience kick in when violent intentions are directed at police officers who are expected to protect potential victims from violence. But yelling and pointing guns is “like pouring gasoline on a fire when you do that with the mentally ill,” said Ron Honberg, policy director with the National Alliance on Mental Illness cited in the Washington Post article on July 1. Mr. Honberg fails to realize that if officers are yelling and pointing firearms it is because the force continuum has already exceeded the level of a shoot-don’t shoot lethal force scenario. The degree of response intensity follows an expected path that is based on the actions of the perpetrator not the actions of the police. The Post integrated video clips from officer involved shootings and the Longview, TX incident depicts how quickly someone with a knife can cover the distance between two officers. Read my published blog on the Myth of Mental Illness as it cites the truly low incidence of crime and violence among those diagnosed with mental illness. (https://msefton.wordpress.com/2015/03/02/the-myth-of-mental-illness-and-school-violence/)
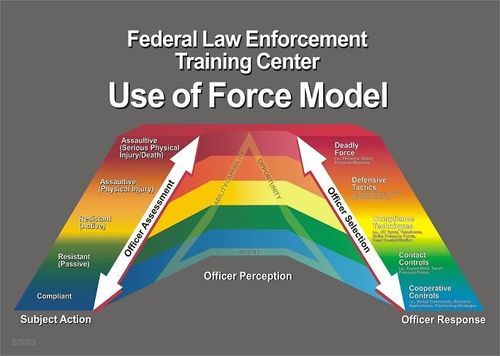
 The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.
The mere fact that someone has mental illness such as schizophrenia, bipolar depression, or anxiety has less to do with whether or not they are at higher risk for lethal force being used against them. Rather, the behavioral context in which they become involved with police officers, i.e. the “nature of the call” is what guides the and officers tactical use of force along a continuum. The use of force continuum is drafted by the National Institute of Justice as a template for guiding the response of officers to tactical scenarios of degrees of resistance exhibited by civilians with whom they come into contact. Verbalization of commands tends to be the most commonly used by police in most encounters with resistant persons. For those individuals who exhibit more defiant and aggressive posture officers are permitted the use of elevated degrees of response (increased use of force) including the deployment of pepper spray and perhaps the deployment of a taser or baton for gaining compliance. A confounding variable in all calls for service – including those where someone wants help for his illness is the co-morbid or co-existing addiction and substance abuse. Its role on crime and violence elevate the threat exponentially.- In a published a blog I have reported that mentally ill persons are no more likely to be violent than individuals without mental illness. However, individuals exhibiting paranoia and those with the acute suicidal ideation are at high risk for acting out violently against police officers and engaging in “suicide by cop” behaviors and place them at greater risk for having lethal force being used against them. There are no single words that will de-escalate someone who has decided on killing themselves or someone else. More importantly, the dynamics of the suicide by cop scenario are a lose-lose for everyone involved – except perhaps the suicidal person who gets what he wants.
- “Nationwide, police have shot and killed 124 people this year who were in the throes of mental or emotional crisis, according to a Washington Post analysis. The dead account for a quarter of the 462 people shot to death by police in the first six months of 2015” (June 30, 2105). This is but a fraction of the number of persons who experience suicidal ideation on a daily basis who do not act out their behavior in such a destruction manner. Published accounts have recently blamed the lack of police officer training in managing psychiatric emergencies as a possible underpinning of increased officer involved shootings of persons exhibiting signs of mental illness. Arguably, as a psychologist who has worked with people in crisis, it is often quite difficult to assess who is most at risk for self-destruction because those who are most dangerous often appear quite sane. 2007 Virginia Tech mass murderer Seung-Hui Cho gave off few clues of his grave intentions before killing 32 innocent students – yet the video taped manifesto left no doubt that he was experiencing significant emotional conflict. Ultimately, Cho had been hospitalized at least once for depression and paranoia but was free to purchase the firearms he used on April 16, 2007 culminating with his frenetic shooting spree and suicide.
- In Los Angeles, CA the police have an active mental health response team that assist police officers on scene by “slowing things down” using trained, persuasive negotiation in an effort to defuse high stress incidents and lower the number of lethal encounters. The program in L.A. seeks greater communication and understanding between the police and members of the mentally ill community, according the the Washington Post. Mary Jo MacArthur is the assistant chief of the L.A. police training program. She teaches that those in crisis do not process information like other persons and may experience fear and anger when given verbal commands they do not understand. The L.A. model provides for professional support from trained psychologists or psychiatrists on scene. But an officer who encounters an impulsive and violent man menacing with a firearm or knife cannot be expected to de-escalate and “slow down” a volatile situation when the threat of lethal force being used against them or someone else exists in real time.
- It is inflammatory to say that police did not handle this case or that case appropriately. The use of force continuum is clear that force is met with similar degree of force in order to control and de-escalate. Any other mismatch of force place everyone in grave danger. Once the lethal threat is neutralized – such as when the mentally ill person drops all weapons and submits to verbal commands to surrender – additional investigation and support may be provided by local mental health teams including hospitalization as needed. Another program exists in Vancouver, B.C. that I will review in my next update.
- Police officers are regarded as the front line first responders to family conflict and crisis. The most volatile scenes are those where mental illness coexists with substance abuse like heroin addiction and domestic conflict. For better or worse, the police have an opportunity to effect change whenever they enter into the domestic foray or crisis involving members of the mentally ill community. This affords them a window into the chaos and the opportunity to bring calm to crisis. In past blogs I have introduced the notion of aftermath intervention as a means to ending the repetitive nature of those in crisis. Added training to deconstruct the myths of mental illness after each encounter may be useful but time is seldom provided for such debriefing. As with many states who review domestic violence homicide – mental health response teams based on the L.A. model and post hoc analysis of red flag indicators of the potential for violence fueled by mental illness i.e. delusions, hallucinations, active PTSD, should be carefully crafted for officer and community safety.
- “Community policing has long espoused the partnership between police and citizens. The positive benefits of this create bridges between the two that may benefit officers at times of need – including the de facto extra set of eyes when serious crimes are reported” (Sefton, 2013). These extra eyes may be called upon to identify red flags as they wave suggesting someone may be headed down the path of destruction. In the case of some noteworthy domestic violence, post hoc analysis often reveals that people were aware that something was going to happen and not a single person stepped up to strike a warning (Allanach, 2011). Police agencies cannot work in a vacuum and must have the help of citizens if they are to have any impact de-escalating the mentally ill prior to onset of terminal rage.
- In many cases, the correct response to intimate partner violence should include aftermath intervention when the crisis has settled from the crisis that brought police to this threshold. Techniques for understanding mental illness may facilitate mutual understanding and establish the needed bridge to facilitate treatment. When this is done it establishes a baseline of trust, empathy, and resilience and may lessen the likelihood of the violent menacing that demands force be met with force regardless of the diagnosis. In the next blog I will identify the role of police officers in pre-incident intervention and identify a chilling case. By the time a person is in crisis there may be little time to talk “sense” and de-escalate no matter how skilled and well trained the police become.
REFERENCES
- Ronald Allanach et al., Psychological Autopsy of June 13, 2011, Dexter, Maine Domestic Violence Homicides and Suicide: Final Report 39 (Nov.28,2011), http://pinetreewatchdog.org/files/2011/12/Dexter-DVH-Psychological-Autopsy-Final-Report-112811-111.pdf
- Lowery, W, Kimberly Kindy, K, Alexander, K. Distraught people – deadly results, Taken June 30, 2015 http://www.washingtonpost.com/sf/investigative/2015/06/30/distraught-people-deadly-results/?hpid=z3
- Sefton, M. (2013) Blog: Aftermath Intervention: Police first to the threshhold. December 8, 2013 Taken June 30, 2015, https://www.msefton.wordpress.com/2013/12/08/aftermath-intervention-police-first-to-the-threshold/


